Srinivasan Neil T, Orini Michele, Simon Ron B, Providência Rui, Khan Fakhar Z, Segal Oliver R, Babu Girish G, Bradley Richard, Rowland Edward, Ahsan Syed, Chow Anthony W, Lowe Martin D, Taggart Peter, Lambiase Pier D
Department of Cardiac Electrophysiology, The Barts Heart Center, St Bartholomew's Hospital, London, United Kingdom; and Institute of Cardiovascular Science, University College London, London, United Kingdom.
Department of Cardiac Electrophysiology, The Barts Heart Center, St Bartholomew's Hospital, London, United Kingdom; and.
Am J Physiol Heart Circ Physiol. 2016 Sep 1;311(3):H545-54. doi: 10.1152/ajpheart.00159.2016. Epub 2016 Jul 1.
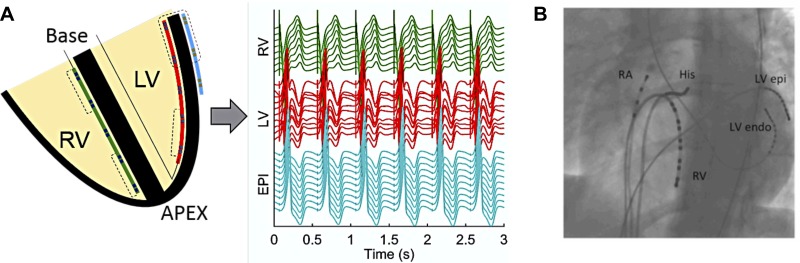
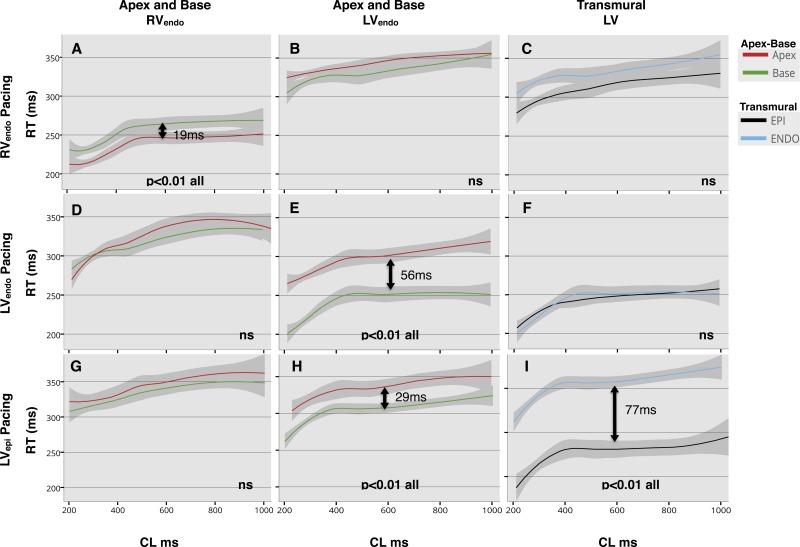
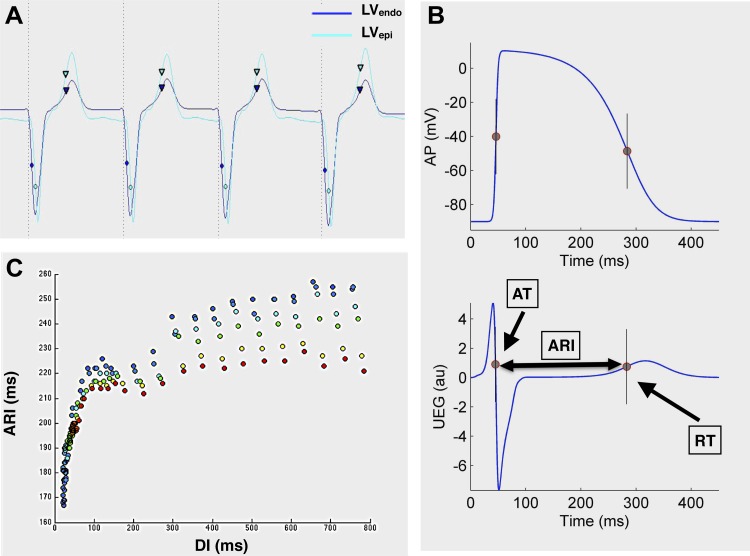
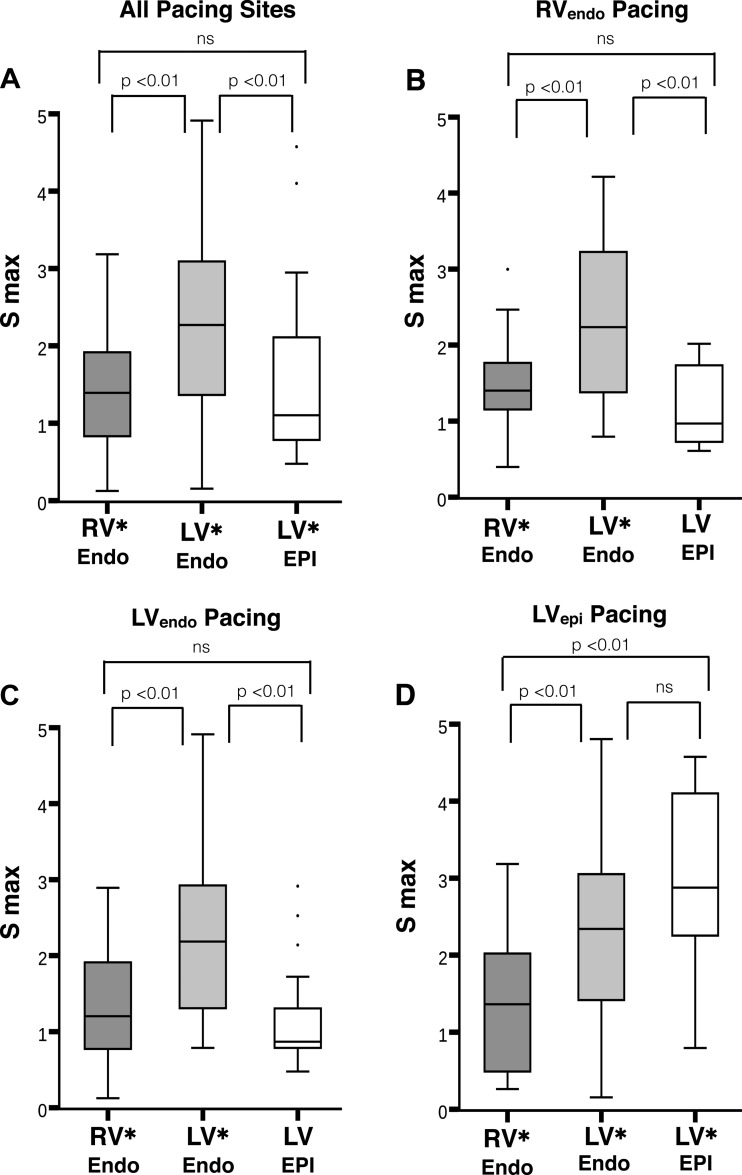
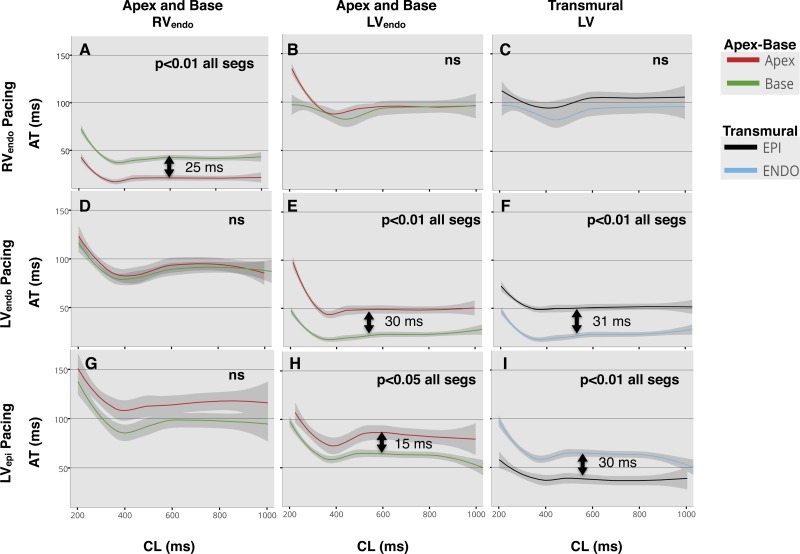
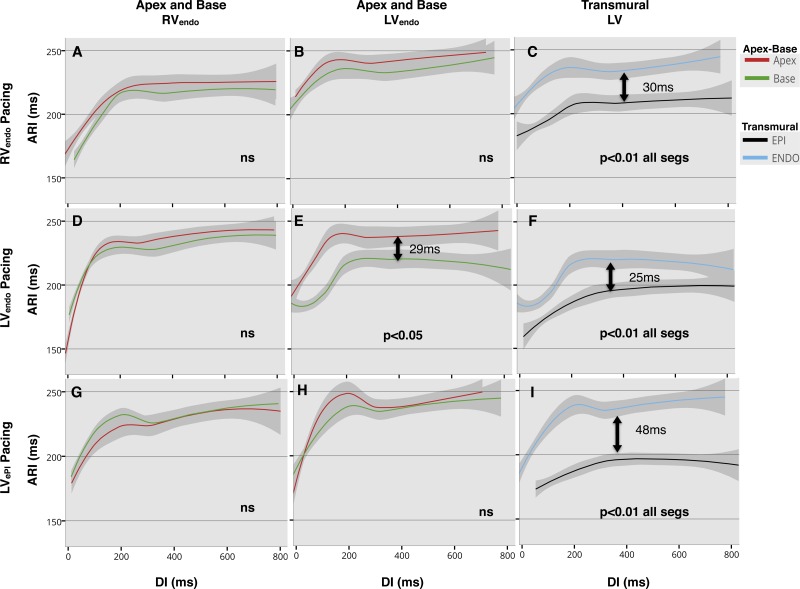
The spatial variation in restitution properties in relation to varying stimulus site is poorly defined. This study aimed to investigate the effect of varying stimulus site on apicobasal and transmural activation time (AT), action potential duration (APD) and repolarization time (RT) during restitution studies in the intact human heart. Ten patients with structurally normal hearts, undergoing clinical electrophysiology studies, were enrolled. Decapolar catheters were placed apex to base in the endocardial right ventricle (RVendo) and left ventricle (LVendo), and an LV branch of the coronary sinus (LVepi) for transmural recording. S1-S2 restitution protocols were performed pacing RVendo apex, LVendo base, and LVepi base. Overall, 725 restitution curves were analyzed, 74% of slopes had a maximum slope of activation recovery interval (ARI) restitution (Smax) > 1 (P < 0.001); mean Smax = 1.76. APD was shorter in the LVepi compared with LVendo, regardless of pacing site (30-ms difference during RVendo pacing, 25-ms during LVendo, and 48-ms during LVepi; 50th quantile, P < 0.01). Basal LVepi pacing resulted in a significant transmural gradient of RT (77 ms, 50th quantile: P < 0.01), due to loss of negative transmural AT-APD coupling (mean slope 0.63 ± 0.3). No significant transmural gradient in RT was demonstrated during endocardial RV or LV pacing, with preserved negative transmural AT-APD coupling (mean slope -1.36 ± 1.9 and -0.71 ± 0.4, respectively). Steep ARI restitution slopes predominate in the normal ventricle and dynamic ARI; RT gradients exist that are modulated by the site of activation. Epicardial stimulation to initiate ventricular activation promotes significant transmural gradients of repolarization that could be proarrhythmic.
关于不同刺激部位的恢复特性的空间变化定义尚不明确。本研究旨在探讨在完整人体心脏的恢复研究中,不同刺激部位对心尖 - 基底部及跨壁激活时间(AT)、动作电位时程(APD)和复极时间(RT)的影响。纳入了10名心脏结构正常且正在接受临床电生理研究的患者。将十极导管从心尖至心底放置于心内膜右心室(RVendo)和左心室(LVendo),并将冠状窦的左心室分支(LVepi)用于跨壁记录。在RVendo心尖、LVendo心底和LVepi心底进行S1 - S2恢复方案起搏。总体而言,分析了725条恢复曲线,74%的斜率具有激活恢复间期(ARI)恢复的最大斜率(Smax)>1(P<0.001);平均Smax = 1.76。无论起搏部位如何,LVepi的APD均短于LVendo(RVendo起搏时相差30毫秒,LVendo起搏时相差25毫秒,LVepi起搏时相差48毫秒;第50百分位数,P<0.01)。由于跨壁AT - APD负耦合的丧失(平均斜率0.63±0.3),LVepi基底起搏导致显著的跨壁RT梯度(77毫秒,第50百分位数:P<0.01)。在心内膜RV或LV起搏期间未显示出显著的跨壁RT梯度,且保留了跨壁AT - APD负耦合(平均斜率分别为 - 1.36±1.9和 - 0.71±0.4)。正常心室和动态ARI中陡峭 的ARI恢复斜率占主导;存在由激活部位调节的RT梯度。启动心室激活的心外膜刺激会促进显著的跨壁复极梯度,这可能是致心律失常的。