Ikonomi Erkanda, Rothstein Robin D, Ehrlich Adam C, Friedenberg Frank K
Department of Medicine, Temple University School of Medicine, Philadelphia, PA.
Temple Inflammatory Bowel Disease Program, Temple University School of Medicine, Philadelphia, PA.
J Gastroenterol Pancreatol Liver Disord. 2016;3(1). doi: 10.15226/2374-815X/3/1/00146. Epub 2016 Jan 27.
Definitive diagnosis of IBD requires endoscopic and pathologic confirmation. These tools are also used to classify disease activity. Our aim was to determine if the fractional exhaled nitric oxide (FeNO) could be utilized to screen for IBD and assess for disease activity.
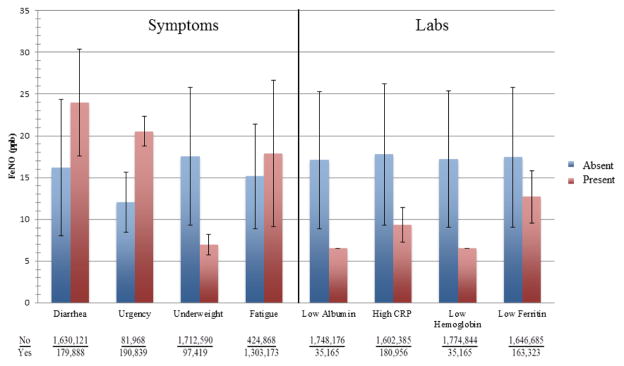
We matched weighted IBD cases and controls from the 2009-2010 NHANES dataset. All subjects underwent measurement of FeNO using standardized techniques. We assessed for potential confounders for FeNO measurement including age, height, and asthma. For IBD subjects, we used the presence of diarrhea, fatigue, and weight loss as a proxy for IBD activity. Laboratory parameters examined to estimate disease activity included anemia (≤ 10 g/dl), iron deficiency (ferritin ≤ 20 ng/ml), hypoalbuminemia (≤ 3.2 g/dl), and CRP (≥ 1.1 mg/dl).
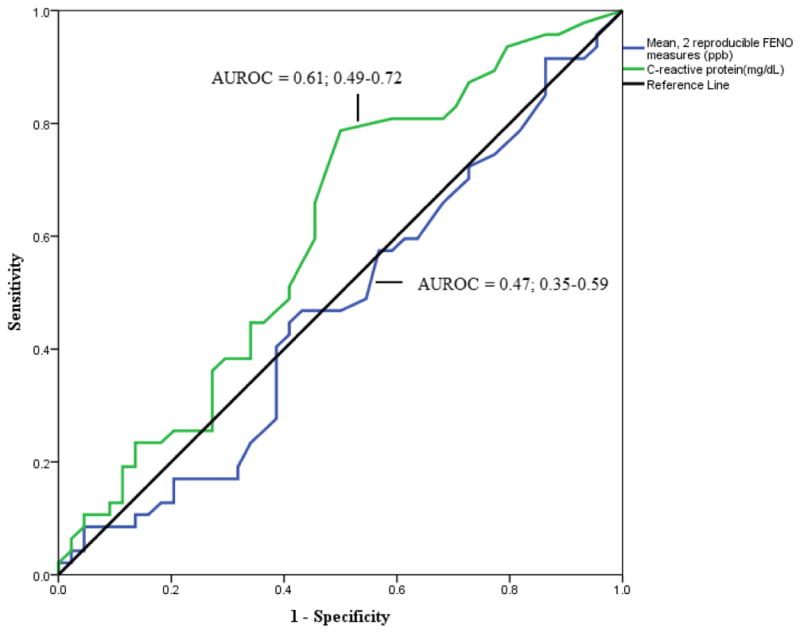
The weighted sample represented 199,414,901 subjects. The weighted prevalence of IBD was 2,084,895 (1.0%). IBD subjects had nearly the same FeNO level as those without IBD (17.0 ± 16.2 vs. 16.7 ± 14.5 ppb). The odds of a FeNO > 25 ppb was half (OR=0.501; 95% CI 0.497-0.504) for subjects with IBD compared to those without IBD after controlling for confounders. The AUROC curve for FeNO was 0.47 (0.35-0.59). FeNO levels were not higher in patients with laboratory values suggestive of active disease. FeNO levels were higher in IBD patients with diarrhea, rectal urgency, and fatigue but were lower in those with unintentional weight loss.
Measurement of FeNO does not appear to be useful to screen for IBD or assess disease activity.
IBD的确诊需要内镜和病理证实。这些工具也用于对疾病活动进行分类。我们的目的是确定呼出一氧化氮分数(FeNO)是否可用于筛查IBD并评估疾病活动。
我们从2009 - 2010年美国国家健康与营养检查调查(NHANES)数据集中匹配了加权的IBD病例和对照。所有受试者均采用标准化技术测量FeNO。我们评估了FeNO测量的潜在混杂因素,包括年龄、身高和哮喘。对于IBD受试者,我们将腹泻、疲劳和体重减轻的存在作为IBD活动的替代指标。为评估疾病活动而检查的实验室参数包括贫血(≤10 g/dl)、缺铁(铁蛋白≤20 ng/ml)、低白蛋白血症(≤3.2 g/dl)和CRP(≥1.1 mg/dl)。
加权样本代表199,414,901名受试者。IBD的加权患病率为2,084,895(1.0%)。IBD受试者的FeNO水平与非IBD受试者几乎相同(17.0±16.2 vs. 16.7±14.5 ppb)。在控制混杂因素后,IBD受试者FeNO>25 ppb的几率是非IBD受试者的一半(OR = 0.501;95% CI 0.497 - 0.504)。FeNO的受试者工作特征曲线下面积(AUROC)为0.47(0.35 - 0.59)。提示疾病活动的实验室值患者的FeNO水平并不更高。腹泻、直肠紧迫感和疲劳的IBD患者FeNO水平较高,但非故意体重减轻的患者FeNO水平较低。
测量FeNO似乎对筛查IBD或评估疾病活动无用。