Kil Whoon Jong, Kulasekere Christina, Derrwaldt Ronald, Bugno Jacob, Hatch Craig
Cleveland Veterans Affairs Medical Center, Cleveland, Ohio, USA.
Oncotarget. 2016 Aug 16;7(33):53029-53036. doi: 10.18632/oncotarget.10621.
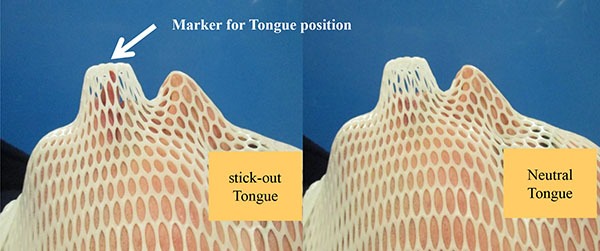
To assess changes in oral cavity (OC) shapes and radiation doses to tongue with different tongue positions during intensity-modulated radiation therapy (IMRT) in patients with head and neck squamous cell carcinoma (HNSCC) but who refused or did not tolerate an intraoral device (IOD), such as bite block, tongue blade, or mouthpiece.
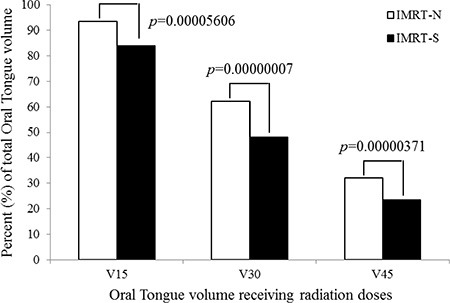
Tongue volume outside of OC was 7.1 ± 3.8 cm3 (5.4 ± 2.6% of entire OC and 7.8 ± 3.1% of oral tongue) in IMRT-S. Dmean of OC was 34.9 ± 8.0 Gy and 31.4 ± 8.7 Gy with IMRT-N and IMRT-S, respectively (p < 0.001). OC volume receiving ≥ 36 Gy (V36) was 40.6 ± 16.9% with IMRT-N and 33.0 ± 17.0% with IMRT-S (p < 0.001). Dmean of tongue was 38.1 ± 7.9 Gy and 32.8 ± 8.8 Gy in IMRT-N and IMRT-S, respectively (p < 0.001). V15, V30, and V45 of tongue were significantly lower in IMRT-S (85.3 ± 15.0%, 50.6 ± 16.2%, 24.3 ± 16.0%, respectively) than IMRT-N (94.4 ± 10.6%, 64.7 ± 16.2%, 34.0 ± 18.6%, respectively) (all p < 0.001). Positional offsets of tongue during the course of IMRT-S was -0.1 ± 0.2 cm, 0.01 ± 0.1 cm, and -0.1 ± 0.2 cm (vertical, longitudinal, and lateral, respectively).
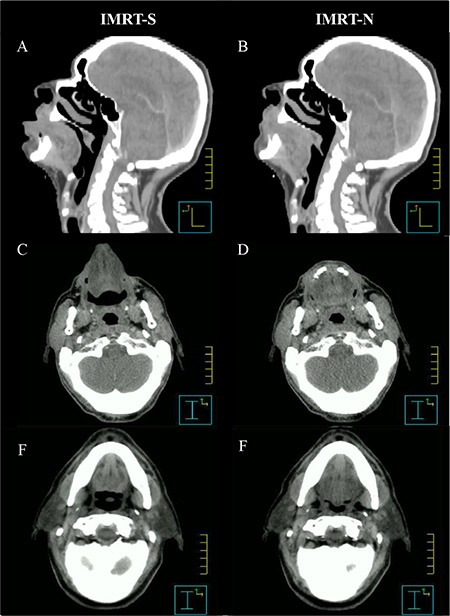
13 patients with HNSCC underwent CT-simulations both with a neutral tongue position and a stick-out tongue for IMRT planning (IMRT-N and IMRT-S, respectively). Planning objectives were to deliver 70 Gy, 63 Gy, and 56 Gy in 35 fractions to 95% of PTVs. Radiation Therapy Oncology Group (RTOG) recommended dose constraints were applied. Data are presented as mean ± standard deviation and compared using the student t-test.
IMRT-S for patients with HNSCC who refused or could not tolerate an IOD has significant decreased radiation dose to the tongue than IMRT-N, which may potentially reduce RT related toxicity in tongue in selected patients.
评估头颈部鳞状细胞癌(HNSCC)患者在调强放射治疗(IMRT)期间,拒绝或无法耐受口腔内装置(IOD)(如咬块、压舌板或口含器)时,口腔(OC)形状的变化以及不同舌位时舌部的辐射剂量。
IMRT-S中,OC外的舌体积为7.1±3.8 cm³(占整个OC的5.4±2.6%,占口腔舌的7.8±3.1%)。IMRT-N和IMRT-S时,OC的平均剂量分别为34.9±8.0 Gy和31.4±8.7 Gy(p<0.001)。接受≥36 Gy(V36)的OC体积,IMRT-N时为40.6±16.9%,IMRT-S时为33.0±17.0%(p<0.001)。IMRT-N和IMRT-S时,舌的平均剂量分别为38.1±7.9 Gy和32.8±8.8 Gy(p<0.001)。IMRT-S时舌的V15、V30和V45显著低于IMRT-N(分别为85.3±15.0%、50.6±16.2%、24.3±16.0%)(分别为94.4±10.6%、64.7±16.2%、34.0±18.6%)(均p<0.001)。IMRT-S过程中舌的位置偏移分别为-0.1±0.2 cm、0.01±(此处原文可能有误,推测是0.1)0.1 cm和-0.1±0.2 cm(分别为垂直、纵向和横向)。
13例HNSCC患者分别在舌处于中立位和伸出位时进行CT模拟,用于IMRT计划(分别为IMRT-N和IMRT-S)。计划目标是在35次分割中向95%的计划靶体积(PTV)给予70 Gy、63 Gy和56 Gy。应用了放射治疗肿瘤学组(RTOG)推荐的剂量限制。数据以平均值±标准差表示,并使用学生t检验进行比较。
对于拒绝或无法耐受IOD的HNSCC患者,IMRT-S比IMRT-N使舌部的辐射剂量显著降低,这可能会降低部分患者舌部放疗相关的毒性。