Ashby Lynn S, Smith Kris A, Stea Baldassarre
Department of Neurology, Barrow Neurological Institute, 500 W. Thomas Rd, Suite 300, Phoenix, AZ, 85013, USA.
Department of Neurosurgery, Barrow Neurological Institute, Phoenix, AZ, 85013, USA.
World J Surg Oncol. 2016 Aug 24;14(1):225. doi: 10.1186/s12957-016-0975-5.
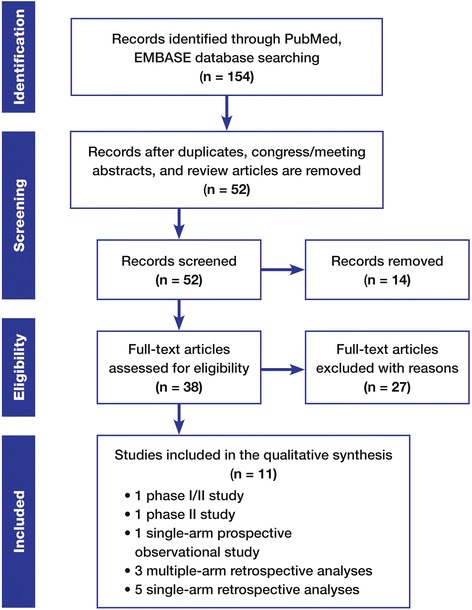
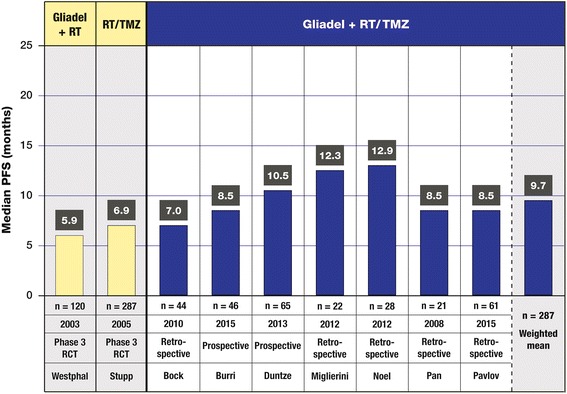
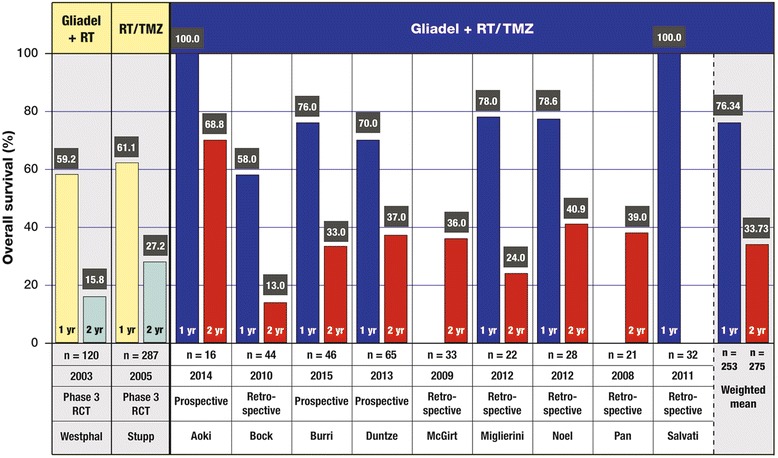
Since 2003, only two chemotherapeutic agents, evaluated in phase III trials, have been approved by the US Food and Drug Administration for treatment of newly diagnosed high-grade glioma (HGG): Gliadel wafers (intracranially implanted local chemotherapy) and temozolomide (TMZ) (systemic chemotherapy). Neither agent is curative, but each has been shown to improve median overall survival (OS) compared to radiotherapy (RT) alone. To date, no phase III trial has tested these agents when used in sequential combination; however, a number of smaller trials have reported favorable results. We performed a systematic literature review to evaluate the combination of Gliadel wafers with standard RT (60 Gy) plus concurrent and adjuvant TMZ (RT/TMZ) for newly diagnosed HGG. A literature search was conducted for the period of January 1995 to September 2015. Data were extracted and categorized, and means and ranges were determined. A total of 11 publications met criteria, three prospective trials and eight retrospective studies, representing 411 patients who received Gliadel plus standard RT/TMZ. Patients were similar in age, gender, and performance status. The weighted mean of median OS was 18.2 months (ten trials, n = 379, range 12.7 to 21.3 months), and the weighted mean of median progression-free survival was 9.7 months (seven trials, n = 287, range 7 to 12.9 months). The most commonly reported grade 3 and 4 adverse events were myelosuppression (10.22 %), neurologic deficit (7.8 %), and healing abnormalities (4.3 %). Adverse events reflected the distinct independent safety profiles of Gliadel wafers and RT/TMZ, with little evidence of enhanced toxicity from their use in sequential combination. In the 11 identified trials, an increased benefit from sequentially combining Gliadel wafers with RT/TMZ was strongly suggested. Median OS tended to be improved by 3 to 4 months beyond that observed for Gliadel wafers or TMZ when used alone in the respective phase III trials. Larger prospective trials of Gliadel plus RT/TMZ are warranted.
自2003年以来,在III期试验中评估的只有两种化疗药物已被美国食品药品监督管理局批准用于治疗新诊断的高级别胶质瘤(HGG):Gliadel薄片(颅内植入局部化疗)和替莫唑胺(TMZ)(全身化疗)。这两种药物都不能治愈疾病,但与单纯放疗(RT)相比,每种药物都已显示可改善中位总生存期(OS)。迄今为止,尚无III期试验对这些药物序贯联合使用进行测试;然而,一些较小规模的试验报告了良好的结果。我们进行了一项系统的文献综述,以评估Gliadel薄片与标准放疗(60 Gy)加同步和辅助TMZ(RT/TMZ)联合用于新诊断的HGG的情况。对1995年1月至2015年9月期间进行了文献检索。提取数据并进行分类,确定均值和范围。共有11篇出版物符合标准,3项前瞻性试验和8项回顾性研究,代表411例接受Gliadel加标准RT/TMZ治疗的患者。患者在年龄、性别和体能状态方面相似。中位OS的加权均值为18.2个月(10项试验,n = 379,范围12.7至21.3个月),中位无进展生存期的加权均值为9.7个月(7项试验,n = 287,范围7至12.9个月)。最常报告的3级和4级不良事件是骨髓抑制(10.22%)、神经功能缺损(7.8%)和愈合异常(4.3%)。不良事件反映了Gliadel薄片和RT/TMZ各自独立的安全性,几乎没有证据表明序贯联合使用会增加毒性。在11项已确定的试验中,强烈提示Gliadel薄片与RT/TMZ序贯联合使用会增加获益。与在各自的III期试验中单独使用Gliadel薄片或TMZ相比,中位OS往往会延长3至4个月。有必要开展更大规模的Gliadel加RT/TMZ的前瞻性试验。