Bundhun Pravesh Kumar, Janoo Girish, Teeluck Abhishek Rishikesh, Huang Wei-Qiang
Institute of Cardiovascular Diseases, the First Affiliated Hospital of Guangxi Medical University, Nanning, Guangxi, 530027, People's Republic of China.
Guangxi Medical University, Nanning, Guangxi, 530027, People's Republic of China.
BMC Cardiovasc Disord. 2016 Sep 2;16(1):169. doi: 10.1186/s12872-016-0347-7.
Guidelines from the American Heart Association/American College of Cardiology recommend a higher dosage of aspirin daily following Percutaneous Coronary Intervention (PCI), whereas guidelines from the European Society of Cardiology recommend a lower dosage. This study aimed to compare the adverse clinical outcomes associated with a low dose and a high dose of aspirin following PCI.
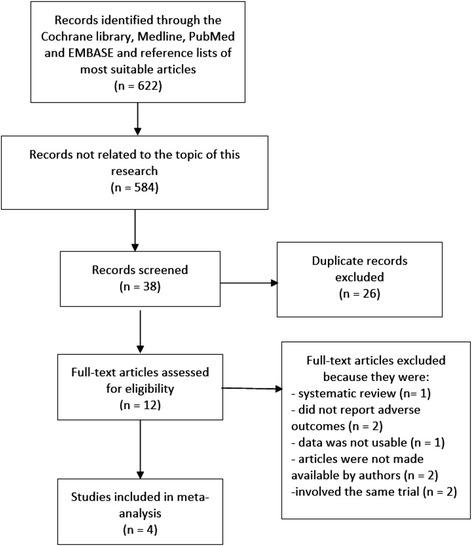
Electronic databases were searched for studies comparing a low dose with a high dose aspirin following PCI. Adverse clinical outcomes were considered as the endpoints in this study. We calculated Odds Ratios (OR) with 95 % Confidence Intervals (CIs) for categorical variables. The pooled analyses were performed with RevMan 5.3 software.
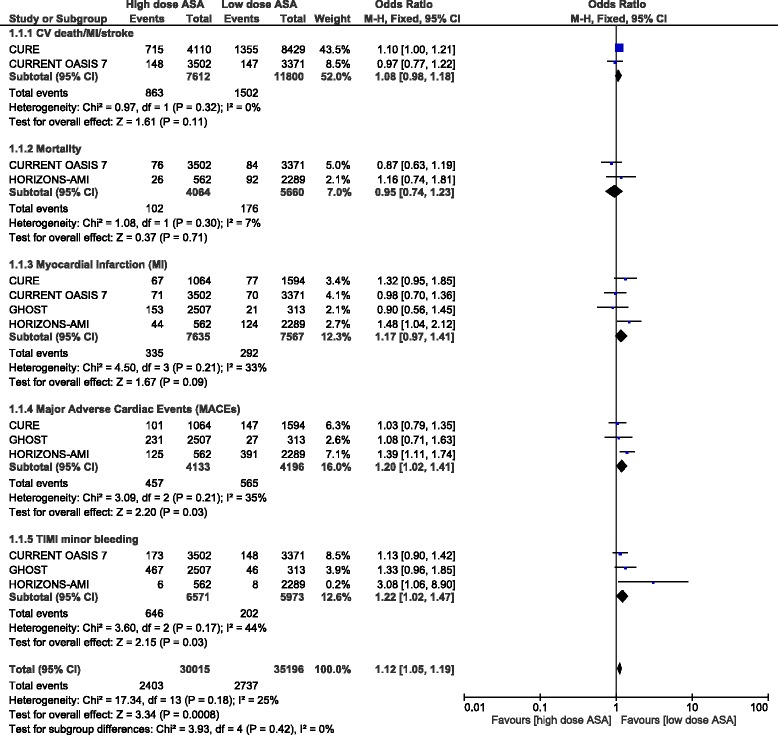
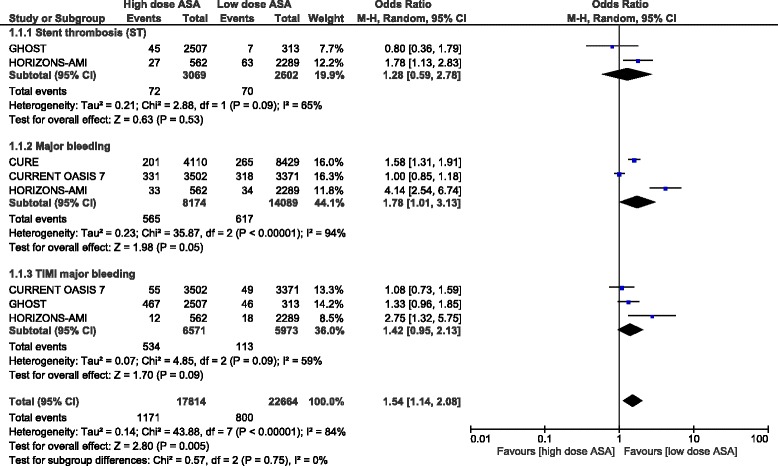
A total number of 25,083 patients were included. Results from this analysis showed that the combination of Cardiovascular (CV) death/Myocardial Infarction (MI) or stroke was not significantly different between a low and high dose of aspirin with OR: 1.08, 95 % CI: 0.98-1.18; P = 0.11. Mortality and MI were also not significantly different between these two treatment regimens following PCI with OR: 0.95, 95 % CI: 0.74-1.23; P = 0.71 and OR: 1.17, 95 % CI: 0.97-1.41; P = 0.09 respectively. However, a high dose of aspirin was associated with a significantly higher rate of Major Adverse Cardiac Events (MACEs) with OR: 1.20, 95 % CI: 1.02-1.41; P = 0.03. Thrombolysis In Myocardial Infarction (TIMI) defined minor bleeding was also significantly higher with a high dose aspirin with OR: 1.22, 95 % CI: 1.02-1.47; P = 0.03. When Stent thrombosis (ST) was compared, no significant difference was found with OR: 1.28, 95 % CI: 0.59-2.58; P = 0.53. Even if TIMI defined major bleeding favored a low dose of aspirin, with OR: 1.42, 95 % CI: 0.95-2.13; P = 0.09, or even if major bleeding was insignificantly higher with a high dose aspirin, with OR: 1.78, 95 % CI: 1.01-3.13; P = 0.05; I(2) = 94 %, higher levels of heterogeneity observed in these subgroups could not be considered significant to any extent.
According to the results of this analysis, a high dose of aspirin following PCI was not associated with any significantly higher rate of CV death/MI/stroke, mortality or MI. However, MACEs significantly favored a low dose of aspirin. In addition, TIMI defined minor bleeding was significantly higher with a high dose of aspirin whereas the results for the major bleeding outcomes were not statistically significant. However, due to limited data availability and since the subgroups analyzing major bleeding were highly heterogeneous, further studies are recommended to completely solve this issue.
美国心脏协会/美国心脏病学会的指南建议经皮冠状动脉介入治疗(PCI)后每日服用较高剂量的阿司匹林,而欧洲心脏病学会的指南则推荐较低剂量。本研究旨在比较PCI后低剂量和高剂量阿司匹林相关的不良临床结局。
检索电子数据库中比较PCI后低剂量和高剂量阿司匹林的研究。本研究将不良临床结局视为终点。对于分类变量,我们计算了比值比(OR)及95%置信区间(CI)。使用RevMan 5.3软件进行汇总分析。
共纳入25,083例患者。该分析结果显示,低剂量和高剂量阿司匹林组中心血管(CV)死亡/心肌梗死(MI)或中风的联合发生率无显著差异,OR为1.08,95%CI为0.98 - 1.18;P = 0.11。PCI后这两种治疗方案的死亡率和MI发生率也无显著差异,OR分别为0.95,95%CI为0.74 - 1.23;P = 0.71以及OR为1.17,95%CI为0.97 - 1.41;P = 0.09。然而,高剂量阿司匹林与主要不良心脏事件(MACE)发生率显著升高相关,OR为1.20,95%CI为1.02 - 1.41;P = 0.03。高剂量阿司匹林组中,心肌梗死溶栓(TIMI)定义的轻微出血发生率也显著更高,OR为1.22,95%CI为1.02 - 1.47;P = 0.03。比较支架血栓形成(ST)时,未发现显著差异,OR为1.28,95%CI为0.59 - 2.58;P = 0.53。即使TIMI定义的严重出血倾向于低剂量阿司匹林,OR为1.42,95%CI为0.95 - 2.13;P = 0.09,或者高剂量阿司匹林组的严重出血发生率虽无显著升高,OR为1.78,95%CI为1.01 - 3.13;P = 0.05;I(2)= 94%,但在这些亚组中观察到的较高异质性在任何程度上都不被认为具有显著性。
根据本分析结果,PCI后高剂量阿司匹林与CV死亡/MI/中风、死亡率或MI的发生率显著升高无关。然而,MACE显著倾向于低剂量阿司匹林。此外,高剂量阿司匹林组中TIMI定义的轻微出血发生率显著更高,而严重出血结局的结果无统计学意义。然而,由于数据可用性有限,且分析严重出血的亚组具有高度异质性,建议进一步研究以彻底解决该问题。