Raghuveer Geetha, White David A, Hayman Laura L, Woo Jessica G, Villafane Juan, Celermajer David, Ward Kenneth D, de Ferranti Sarah D, Zachariah Justin
Circulation. 2016 Oct 18;134(16):e336-e359. doi: 10.1161/CIR.0000000000000443. Epub 2016 Sep 12.
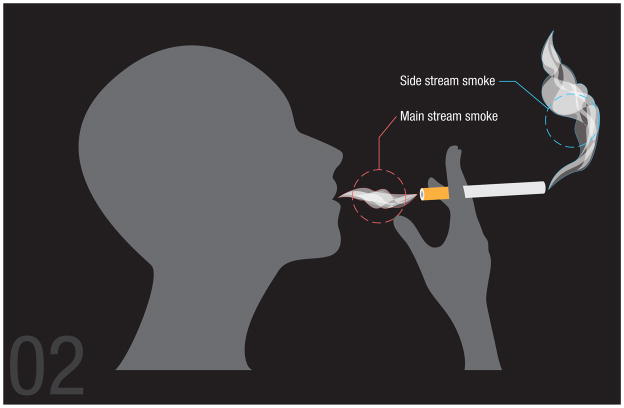
Although public health programs have led to a substantial decrease in the prevalence of tobacco smoking, the adverse health effects of tobacco smoke exposure are by no means a thing of the past. In the United States, 4 of 10 school-aged children and 1 of 3 adolescents are involuntarily exposed to secondhand tobacco smoke (SHS), with children of minority ethnic backgrounds and those living in low-socioeconomic-status households being disproportionately affected (68% and 43%, respectively). Children are particularly vulnerable, with little control over home and social environment, and lack the understanding, agency, and ability to avoid SHS exposure on their own volition; they also have physiological or behavioral characteristics that render them especially susceptible to effects of SHS. Side-stream smoke (the smoke emanating from the burning end of the cigarette), a major component of SHS, contains a higher concentration of some toxins than mainstream smoke (inhaled by the smoker directly), making SHS potentially as dangerous as or even more dangerous than direct smoking. Compelling animal and human evidence shows that SHS exposure during childhood is detrimental to arterial function and structure, resulting in premature atherosclerosis and its cardiovascular consequences. Childhood SHS exposure is also related to impaired cardiac autonomic function and changes in heart rate variability. In addition, childhood SHS exposure is associated with clustering of cardiometabolic risk factors such as obesity, dyslipidemia, and insulin resistance. Individualized interventions to reduce childhood exposure to SHS are shown to be at least modestly effective, as are broader-based policy initiatives such as community smoking bans and increased taxation.
The purpose of this statement is to summarize the available evidence on the cardiovascular health consequences of childhood SHS exposure; this will support ongoing efforts to further reduce and eliminate SHS exposure in this vulnerable population. This statement reviews relevant data from epidemiological studies, laboratory-based experiments, and controlled behavioral trials concerning SHS and cardiovascular disease risk in children. Information on the effects of SHS exposure on the cardiovascular system in animal and pediatric studies, including vascular disruption and platelet activation, oxidation and inflammation, endothelial dysfunction, increased vascular stiffness, changes in vascular structure, and autonomic dysfunction, is examined.
The epidemiological, observational, and experimental evidence accumulated to date demonstrates the detrimental cardiovascular consequences of SHS exposure in children.
Increased awareness of the adverse, lifetime cardiovascular consequences of childhood SHS may facilitate the development of innovative individual, family-centered, and community health interventions to reduce and ideally eliminate SHS exposure in the vulnerable pediatric population. This evidence calls for a robust public health policy that embraces zero tolerance of childhood SHS exposure.
尽管公共卫生项目已使吸烟率大幅下降,但接触烟草烟雾对健康的不良影响绝非过去之事。在美国,十分之四的学龄儿童和三分之一的青少年非自愿接触二手烟草烟雾(SHS),少数族裔背景的儿童以及生活在社会经济地位低下家庭的儿童受影响的比例尤其高(分别为68%和43%)。儿童特别容易受到影响,他们几乎无法控制家庭和社会环境,并且缺乏自行避免接触SHS的理解、能力和自主性;他们还具有一些生理或行为特征,使他们特别容易受到SHS影响。侧流烟雾(从香烟燃烧端冒出的烟雾)是SHS的主要成分,其某些毒素的浓度高于主流烟雾(吸烟者直接吸入的烟雾),这使得SHS可能与直接吸烟一样危险甚至更危险。有力的动物和人体证据表明,儿童时期接触SHS会损害动脉功能和结构,导致过早出现动脉粥样硬化及其心血管后果。儿童时期接触SHS还与心脏自主神经功能受损和心率变异性改变有关。此外,儿童时期接触SHS与肥胖、血脂异常和胰岛素抵抗等心血管代谢危险因素的聚集有关。事实表明,减少儿童接触SHS的个体化干预措施至少有一定效果,社区禁烟和提高税收等更广泛的政策举措也是如此。
本声明的目的是总结关于儿童接触SHS对心血管健康影响的现有证据;这将支持为进一步减少和消除这一弱势群体接触SHS而正在进行的努力。本声明回顾了流行病学研究、基于实验室的实验以及关于SHS与儿童心血管疾病风险的对照行为试验的相关数据。研究了动物和儿科研究中关于SHS接触对心血管系统影响的信息(包括血管破坏和血小板活化、氧化和炎症、内皮功能障碍、血管硬度增加、血管结构变化以及自主神经功能障碍)。
迄今为止积累的流行病学、观察性和实验性证据表明,儿童接触SHS会对心血管产生有害影响。
提高对儿童接触SHS会产生终身不良心血管后果的认识,可能有助于制定创新的个人、以家庭为中心和社区健康干预措施,以减少并理想地消除弱势儿科人群接触SHS的情况。这一证据呼吁制定一项对儿童接触SHS零容忍的强有力公共卫生政策。