Peterson Ingrid, Bar-Zeev Naor, Kennedy Neil, Ho Antonia, Newberry Laura, SanJoaquin Miguel A, Menyere Mavis, Alaerts Maaike, Mapurisa Gugulethu, Chilombe Moses, Mambule Ivan, Lalloo David G, Anderson Suzanne T, Katangwe Thembi, Cunliffe Nigel, Nagelkerke Nico, McMorrow Meredith, Widdowson Marc-Allain, French Neil, Everett Dean, Heyderman Robert S
Malawi-Liverpool-Wellcome Trust.
Institute of Infection and Global Health.
J Infect Dis. 2016 Dec 1;214(11):1700-1711. doi: 10.1093/infdis/jiw426. Epub 2016 Sep 13.
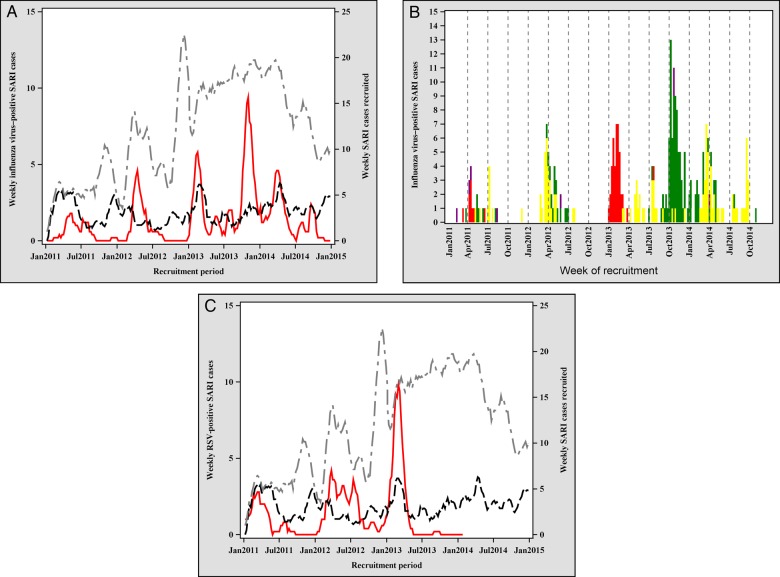
We used data from 4 years of pediatric severe acute respiratory illness (SARI) sentinel surveillance in Blantyre, Malawi, to identify factors associated with clinical severity and coviral clustering.
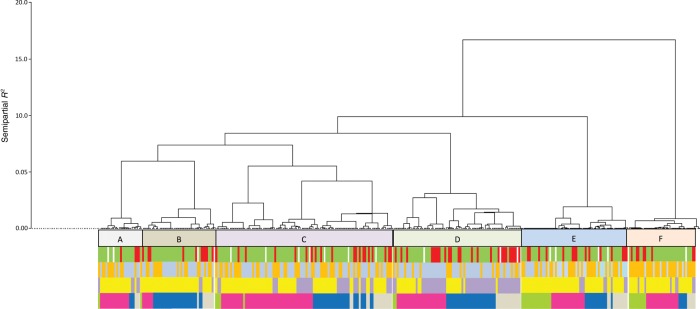
From January 2011 to December 2014, 2363 children aged 3 months to 14 years presenting to the hospital with SARI were enrolled. Nasopharyngeal aspirates were tested for influenza virus and other respiratory viruses. We assessed risk factors for clinical severity and conducted clustering analysis to identify viral clusters in children with viral codetection.
Hospital-attended influenza virus-positive SARI incidence was 2.0 cases per 10 000 children annually; it was highest among children aged <1 year (6.3 cases per 10 000), and human immunodeficiency virus (HIV)-infected children aged 5-9 years (6.0 cases per 10 000). A total of 605 SARI cases (26.8%) had warning signs, which were positively associated with HIV infection (adjusted risk ratio [aRR], 2.4; 95% confidence interval [CI], 1.4-3.9), respiratory syncytial virus infection (aRR, 1.9; 95% CI, 1.3-3.0) and rainy season (aRR, 2.4; 95% CI, 1.6-3.8). We identified 6 coviral clusters; 1 cluster was associated with SARI with warning signs.
Influenza vaccination may benefit young children and HIV-infected children in this setting. Viral clustering may be associated with SARI severity; its assessment should be included in routine SARI surveillance.
我们利用马拉维布兰太尔4年的儿科严重急性呼吸道疾病(SARI)哨点监测数据,以确定与临床严重程度和病毒共检出聚类相关的因素。
2011年1月至2014年12月,纳入2363名3个月至14岁因SARI到医院就诊的儿童。对鼻咽抽吸物进行流感病毒和其他呼吸道病毒检测。我们评估了临床严重程度的危险因素,并进行聚类分析以确定病毒共检出儿童中的病毒聚类。
医院就诊的流感病毒阳性SARI发病率为每年每10000名儿童2.0例;在<1岁儿童中最高(每10000名儿童6.3例),在5-9岁感染人类免疫缺陷病毒(HIV)的儿童中为每10000名儿童6.0例。共有605例SARI病例(26.8%)有警示体征,其与HIV感染(调整风险比[aRR],2.4;95%置信区间[CI],1.4-3.9)、呼吸道合胞病毒感染(aRR,1.9;95%CI,1.3-3.0)和雨季(aRR,2.4;95%CI,1.6-3.8)呈正相关。我们确定了6个病毒共检出聚类;1个聚类与有警示体征的SARI相关。
在这种情况下,流感疫苗接种可能使幼儿和HIV感染儿童受益。病毒聚类可能与SARI严重程度相关;其评估应纳入常规SARI监测。