Mtenga Sally Mmanyi, Geubbels Eveline, Tanner Marcel, Merten Sonja, Pfeiffer Constanze
Ifakara Health Institute (IHI), Ifakara, Tanzania.
Swiss Tropical and Public Health Institute (Swiss TPH), Basel, Switzerland.
Glob Health Action. 2016 Sep 14;9:32326. doi: 10.3402/gha.v9.32326. eCollection 2016.
Behavioral change approaches for human immunodeficiency virus (HIV) prevention in Tanzania encourage married partners to observe safe sex practices (condom use, avoidance of, or safe sex with multiple partners). To implement this advice, partners need to communicate with each other about safer sex, which is often challenging. Although social-structural factors are crucial in understanding sexual behavior, only a few studies focus on understanding safer sex dialogue in a broader social context.
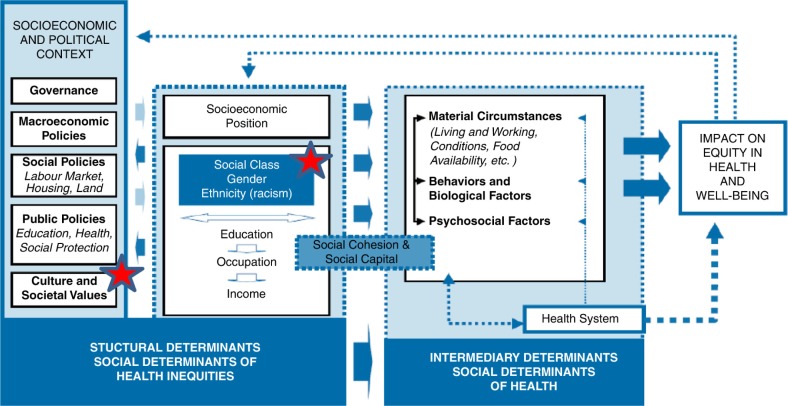
Drawing on the WHO-Commission on the Social Determinants of Health (WHO-CSDH) framework, this study explored key social-structural constructs for studying health in the context of improving safer sex dialogue between polygamous and monogamous partners. Twenty-four in-depth interviews (IDIs) and six focus group discussions (FGDs) with 38 men and women aged 18-60 years were conducted in Ifakara town located in Kilombero district, Tanzania. The study was nested within the community health surveillance project MZIMA (Kiswahili: 'being healthy'). Partners' experiences of safer sex dialogue in polygamous and monogamous relations were investigated and the challenges to safer sex dialogue explored.
The study revealed that open safer sex dialogue in marriage is limited and challenged by social norms about marriage (a view that safer sex dialogue imply that partners are 'not really' married); marital status (a belief that safer sex dialogue is not practical in polygamous marriages, the elder wife should be exempted from the dialogue since she is at lower risk of engaging in extramarital affairs); relationship quality (marital conflicts, extramarital affairs, trust, and sexual dissatisfaction); and gender power relations (the notion that females' initiative to discuss condom use and HIV couple counseling and testing may lead to conflict or divorce).
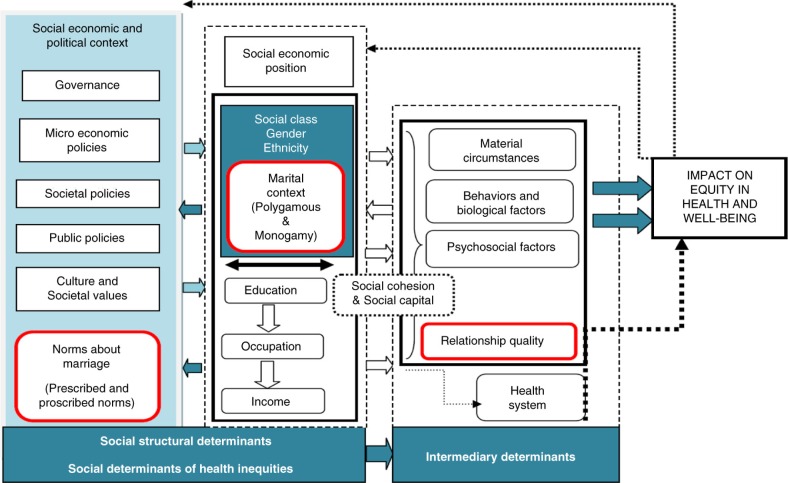
Implementing safer sex practices requires interventions beyond promotion messages. HIV prevention interventions in Tanzania should be carefully adapted to the local context including respective social norms, gender systems, marital context and relationship uncertainties as aspects that facilitate or hinder safer sex dialogue between partners. The WHO-CSDH framework could be strengthened by explicitly integrating relationship quality, marital status, and social norms as additional determinants of health.
坦桑尼亚预防人类免疫缺陷病毒(HIV)的行为改变方法鼓励已婚伴侣遵守安全性行为规范(使用避孕套、避免与多个伴侣发生性行为或与多个伴侣进行安全性行为)。为了落实这一建议,伴侣之间需要就更安全性行为进行沟通,而这通常具有挑战性。尽管社会结构因素对于理解性行为至关重要,但只有少数研究关注在更广泛的社会背景下理解更安全性行为对话。
本研究借鉴世界卫生组织健康问题社会决定因素委员会(WHO-CSDH)的框架,探讨了在改善一夫多妻制和一夫一妻制伴侣之间更安全性行为对话的背景下研究健康的关键社会结构要素。在坦桑尼亚基洛梅罗区的伊法卡拉镇,对38名年龄在18至60岁之间的男性和女性进行了24次深入访谈(IDI)和6次焦点小组讨论(FGD)。该研究嵌套于社区健康监测项目MZIMA(斯瓦希里语:“保持健康”)之中。调查了伴侣在一夫多妻制和一夫一妻制关系中更安全性行为对话的经历,并探讨了更安全性行为对话面临的挑战。
研究表明,婚姻中公开的更安全性行为对话有限,并受到有关婚姻的社会规范(认为更安全性行为对话意味着伴侣“并非真正”结婚)、婚姻状况(认为更安全性行为对话在一夫多妻制婚姻中不实际,年长的妻子应免于对话,因为她婚外情风险较低)、关系质量(婚姻冲突、婚外情、信任和性方面的不满)以及性别权力关系(认为女性主动讨论使用避孕套以及HIV伴侣咨询和检测可能导致冲突或离婚)的挑战。
实施更安全性行为规范需要超越宣传信息的干预措施。坦桑尼亚的HIV预防干预措施应根据当地情况进行精心调整,包括各自的社会规范、性别制度、婚姻背景以及关系的不确定性等促进或阻碍伴侣之间更安全性行为对话的方面。通过明确将关系质量、婚姻状况和社会规范作为健康的额外决定因素,可以加强WHO-CSDH框架。