Houldcroft Charlotte J, Bryant Josephine M, Depledge Daniel P, Margetts Ben K, Simmonds Jacob, Nicolaou Stephanos, Tutill Helena J, Williams Rachel, Worth Austen J J, Marks Stephen D, Veys Paul, Whittaker Elizabeth, Breuer Judith
Infection, Immunity, Inflammation and Physiological Medicine, Institute of Child Health, University College LondonLondon, UK; Division of Infection and Immunity, University College LondonLondon, UK.
Division of Infection and Immunity, University College London London, UK.
Front Microbiol. 2016 Sep 9;7:1317. doi: 10.3389/fmicb.2016.01317. eCollection 2016.
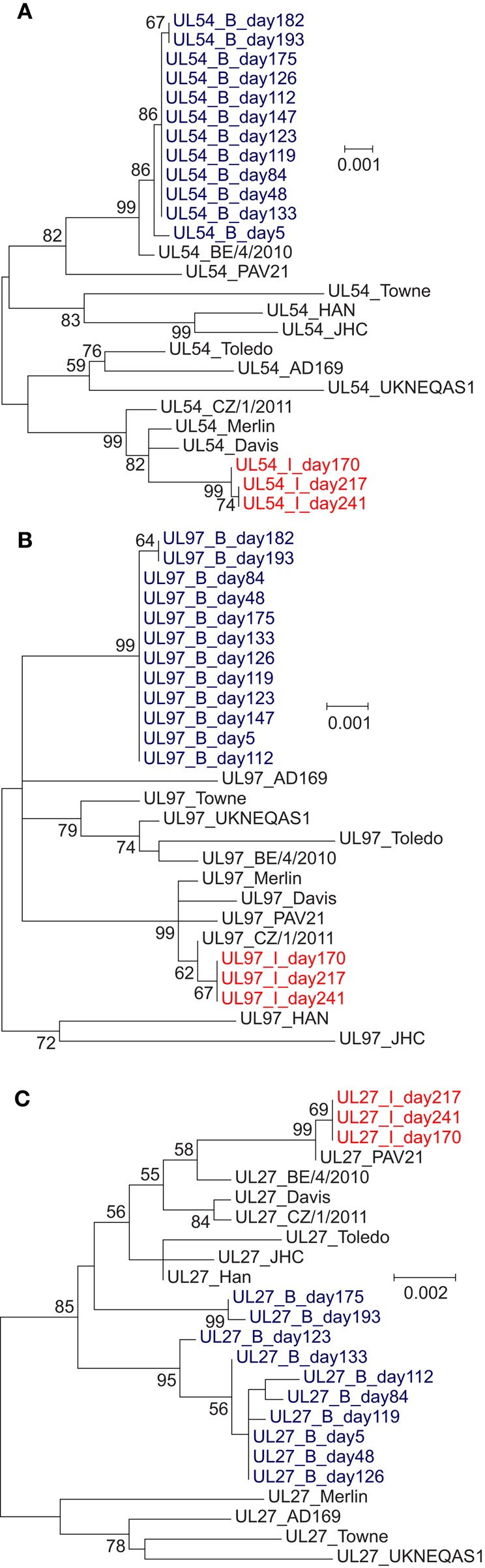
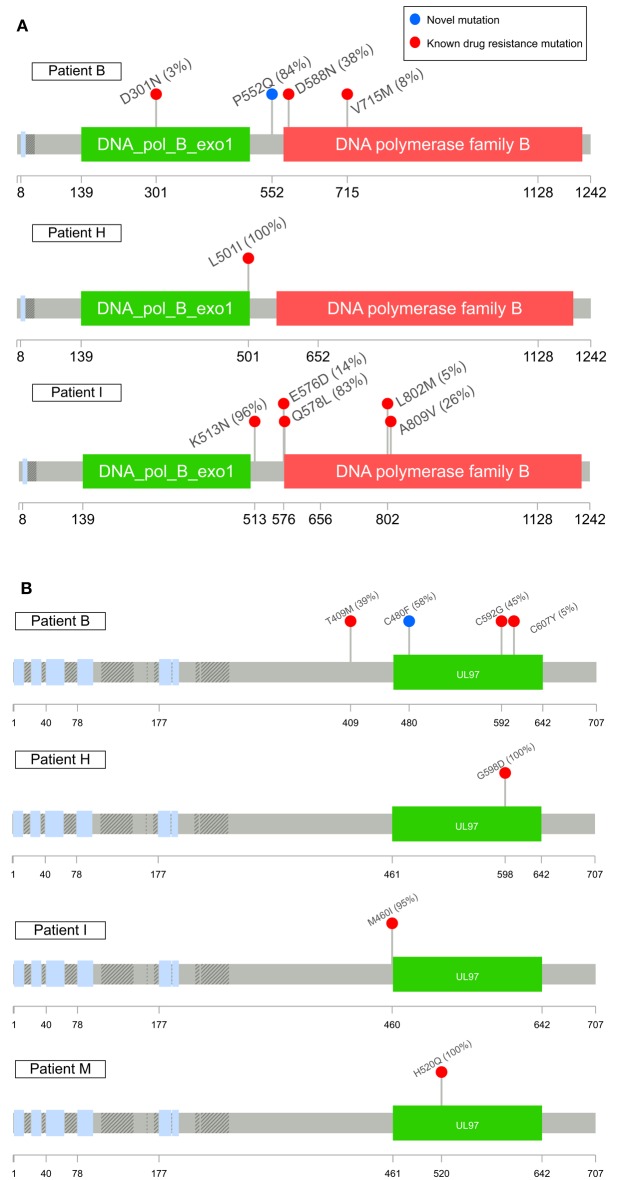
Human cytomegalovirus (HCMV) is a significant pathogen in immunocompromised individuals, with the potential to cause fatal pneumonitis and colitis, as well as increasing the risk of organ rejection in transplant patients. With the advent of new anti-HCMV drugs there is therefore considerable interest in using virus sequence data to monitor emerging resistance to antiviral drugs in HCMV viraemia and disease, including the identification of putative new mutations. We used target-enrichment to deep sequence HCMV DNA from 11 immunosuppressed pediatric patients receiving single or combination anti-HCMV treatment, serially sampled over 1-27 weeks. Changes in consensus sequence and resistance mutations were analyzed for three ORFs targeted by anti-HCMV drugs and the frequencies of drug resistance mutations monitored. Targeted-enriched sequencing of clinical material detected mutations occurring at frequencies of 2%. Seven patients showed no evidence of drug resistance mutations. Four patients developed drug resistance mutations a mean of 16 weeks after starting treatment. In two patients, multiple resistance mutations accumulated at frequencies of 20% or less, including putative maribavir and ganciclovir resistance mutations P522Q (UL54) and C480F (UL97). In one patient, resistance was detected 14 days earlier than by PCR. Phylogenetic analysis suggested recombination or superinfection in one patient. Deep sequencing of HCMV enriched from clinical samples excluded resistance in 7 of 11 subjects and identified resistance mutations earlier than conventional PCR-based resistance testing in 2 patients. Detection of multiple low level resistance mutations was associated with poor outcome.
人巨细胞病毒(HCMV)是免疫功能低下个体中的一种重要病原体,有可能导致致命性肺炎和结肠炎,还会增加移植患者器官排斥的风险。因此,随着新型抗HCMV药物的出现,利用病毒序列数据来监测HCMV病毒血症和疾病中对抗病毒药物新出现的耐药性,包括鉴定假定的新突变,引起了人们极大的兴趣。我们采用靶向富集技术对11名接受单药或联合抗HCMV治疗的免疫抑制儿科患者的HCMV DNA进行深度测序,在1至27周内进行连续采样。分析了抗HCMV药物靶向的三个开放阅读框(ORF)的共有序列变化和耐药突变,并监测耐药突变的频率。对临床材料进行靶向富集测序检测到频率为2%的突变。7名患者未显示耐药突变的证据。4名患者在开始治疗后平均16周出现耐药突变。在两名患者中,多个耐药突变以20%或更低的频率累积,包括假定的马里巴韦和更昔洛韦耐药突变P522Q(UL54)和C480F(UL97)。在一名患者中,比通过聚合酶链反应(PCR)检测到耐药性早14天。系统发育分析表明一名患者存在重组或双重感染。对临床样本中富集的HCMV进行深度测序排除了11名受试者中7人的耐药性,并在两名患者中比基于传统PCR的耐药性检测更早地鉴定出耐药突变。检测到多个低水平耐药突变与不良预后相关。