Rice T W, Lerut T E M R, Orringer M B, Chen L-Q, Hofstetter W L, Smithers B M, Rusch V W, van Lanschot J, Chen K N, Davies A R, D'Journo X B, Kesler K A, Luketich J D, Ferguson M K, Räsänen J V, van Hillegersberg R, Fang W, Durand L, Allum W H, Cecconello I, Cerfolio R J, Pera M, Griffin S M, Burger R, Liu J-F, Allen M S, Law S, Watson T J, Darling G E, Scott W J, Duranceau A, Denlinger C E, Schipper P H, Ishwaran H, Apperson-Hansen C, DiPaola L M, Semple M E, Blackstone E H
Cleveland Clinic, Cleveland, Ohio, USA.
University Ziekenhuizen Leuven, Leuven, Belgium.
Dis Esophagus. 2016 Oct;29(7):715-723. doi: 10.1111/dote.12513.
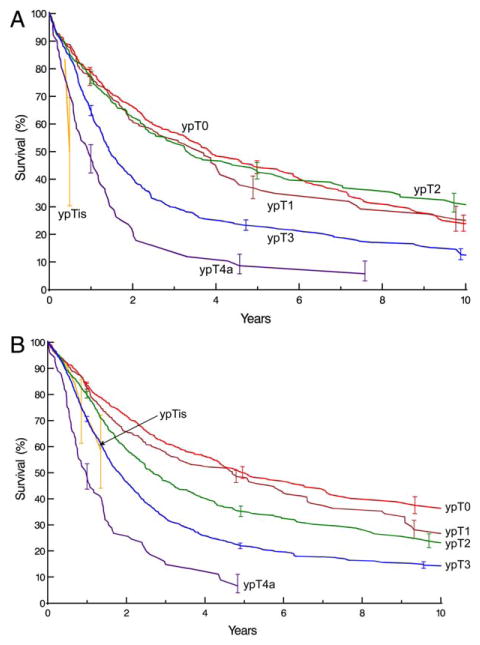
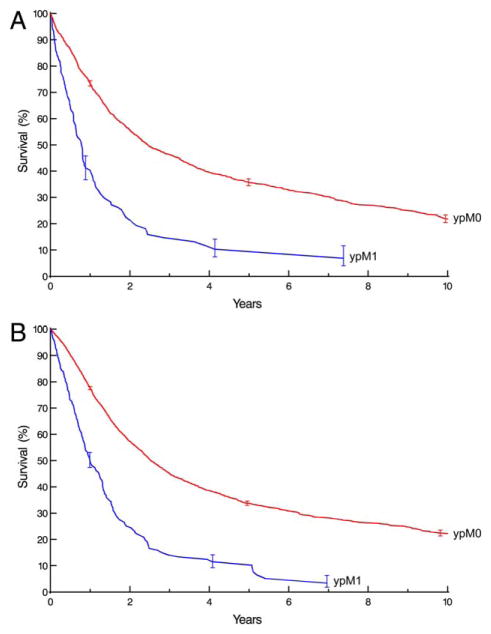
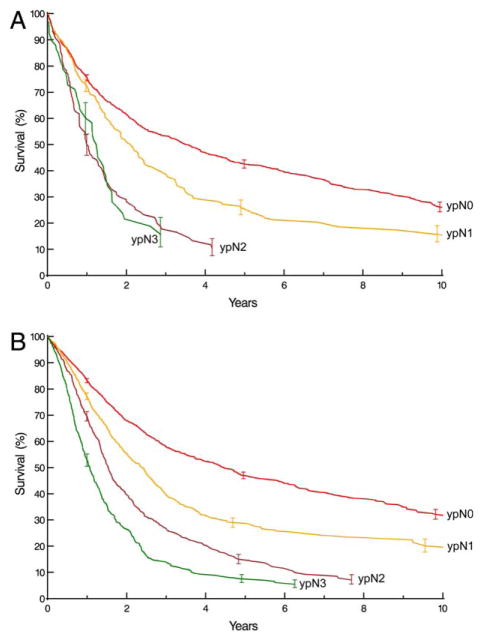
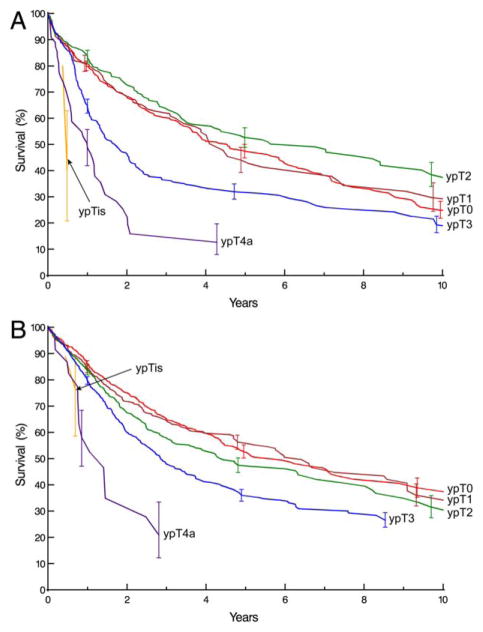
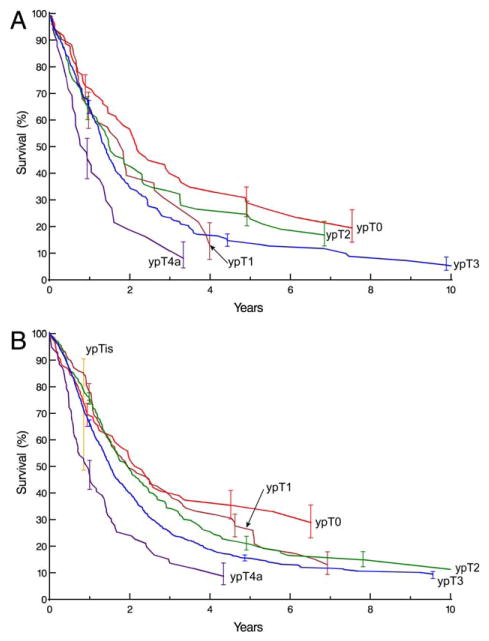
To address uncertainty of whether pathologic stage groupings after neoadjuvant therapy (ypTNM) for esophageal cancer share prognostic implications with pathologic groupings after esophagectomy alone (pTNM), we report data-simple descriptions of patient characteristics, cancer categories, and non-risk-adjusted survival-for pathologically staged cancers after neoadjuvant therapy from the Worldwide Esophageal Cancer Collaboration (WECC). Thirty-three institutions from six continents submitted data using variables with standard definitions: demographics, comorbidities, clinical cancer categories, and all-cause mortality from first management decision. Of 7,773 pathologically staged neoadjuvant patients, 2,045 had squamous cell carcinoma, 5,686 adenocarcinoma, 31 adenosquamous carcinoma, and 11 undifferentiated carcinoma. Patients were older (61 years) men (83%) with normal (40%) or overweight (35%) body mass index, 0-1 Eastern Cooperative Oncology Group performance status (96%), and a history of smoking (69%). Cancers were ypT0 (20%), ypT1 (13%), ypT2 (18%), ypT3 (44%), ypN0 (55%), ypM0 (94%), and G2-G3 (72%); most involved the distal esophagus (80%). Non-risk-adjusted survival for yp categories was unequally depressed, more for earlier categories than later, compared with equivalent categories from prior WECC data for esophagectomy-alone patients. Thus, survival of patients with ypT0-2N0M0 cancers was intermediate and similar regardless of ypT; survival for ypN+ cancers was poor. Because prognoses for ypTNM and pTNM categories are dissimilar, prognostication should be based on separate ypTNM categories and groupings. These data will be the basis for the 8th edition cancer staging manuals following risk adjustment for patient, cancer, and treatment characteristics and should direct 9th edition data collection.
为了探讨食管癌新辅助治疗后的病理分期分组(ypTNM)与单纯食管切除术后的病理分组(pTNM)是否具有相同的预后意义,我们报告了来自全球食管癌协作组(WECC)的新辅助治疗后病理分期癌症患者特征、癌症类别及非风险调整生存情况的简单数据描述。来自六大洲的33个机构使用标准定义的变量提交了数据:人口统计学、合并症、临床癌症类别以及首次治疗决策后的全因死亡率。在7773例新辅助治疗后病理分期的患者中,2045例为鳞状细胞癌,5686例为腺癌,31例为腺鳞癌,11例为未分化癌。患者多为61岁男性(83%),体重指数正常(40%)或超重(35%),东部肿瘤协作组体能状态为0 - 1(96%),有吸烟史(69%)。癌症分期为ypT0(20%)、ypT1(13%)、ypT2(18%)、ypT3(44%)、ypN0(55%)、ypM0(94%),组织学分级为G2 - G3(72%);大多数病变位于食管远端(80%)。与WECC之前单纯食管切除术患者的等效分期相比,yp分期的非风险调整生存率均明显降低,早期分期比晚期分期降低更明显。因此,ypT0 - 2N0M0癌症患者的生存率中等且与ypT无关;ypN + 癌症患者的生存率较差。由于ypTNM和pTNM分期的预后不同,预后判断应基于单独的ypTNM类别和分组。这些数据将作为根据患者、癌症和治疗特征进行风险调整后的第8版癌症分期手册的基础,并指导第9版数据收集。