White Ellen, Smit Erasmus, Churchill Duncan, Collins Simon, Booth Clare, Tostevin Anna, Sabin Caroline, Pillay Deenan, Dunn David T
MRC Clinical Trials Unit at UCL.
Public Health England, Birmingham Heartlands Hospital.
J Infect Dis. 2016 Nov 1;214(9):1302-1308. doi: 10.1093/infdis/jiw213. Epub 2016 May 24.
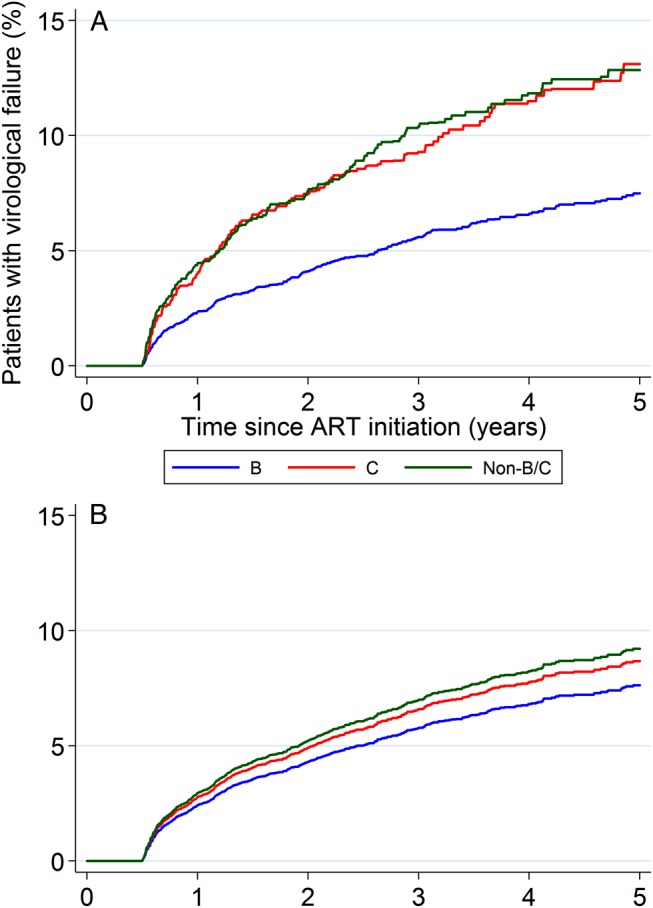
Concern has been expressed that tenofovir-containing regimens may have reduced effectiveness in the treatment of human immunodeficiency virus type 1 (HIV-1) subtype C infections because of a propensity for these viruses to develop a key tenofovir-associated resistance mutation. We evaluated whether subtype influenced rates of virological failure in a cohort of 8746 patients from the United Kingdom who received a standard tenofovir-containing first-line regimen and were followed for a median of 3.3 years. In unadjusted analyses, the rate of failure was approximately 2-fold higher among patients infected with subtype C virus as compared to those with subtype B virus (hazard ratio [HR], 1.86; 95% confidence interval [CI], 1.50-2.31; P < .001). However, the increased risk was greatly attenuated in analyses adjusting for demographic and clinical factors (adjusted HR, 1.14; 95% CI, .83-1.58; P = .41). There were no differences between subtypes C and subtypes non-B and non-C in either univariate or multivariate analysis. These observations imply there is no intrinsic effect of viral subtype on the efficacy of tenofovir-containing regimens.
有人担心,由于感染1型人类免疫缺陷病毒(HIV-1)C亚型的病毒易于出现与替诺福韦相关的关键耐药突变,含替诺福韦的治疗方案在治疗该亚型感染时可能疗效降低。我们评估了病毒亚型是否会影响来自英国的8746例患者的病毒学失败率,这些患者接受了含替诺福韦的标准一线治疗方案,且随访时间中位数为3.3年。在未经校正的分析中,感染C亚型病毒的患者的失败率比感染B亚型病毒的患者高约2倍(风险比[HR],1.86;95%置信区间[CI],1.50 - 2.31;P <.001)。然而,在对人口统计学和临床因素进行校正的分析中,增加的风险大幅降低(校正后HR,1.14;95% CI,.83 - 1.58;P = 0.41)。在单变量或多变量分析中,C亚型与非B非C亚型之间均无差异。这些观察结果表明,病毒亚型对含替诺福韦治疗方案的疗效没有内在影响。