Lee Sang-Min, Lee Jae Hyuk, Kim Kyuseok, Jo You Hwan, Lee Jungyoup, Kim Joonghee, Hwang Ji Eun, Ko Young Sang, Ha Chulmin, Jang Sujin, Park Hyunmi
Department of Emergency Medicine, Seoul National University Bundang Hospital, Seongnam, Korea.
Clin Exp Emerg Med. 2016 Sep 30;3(3):139-147. doi: 10.15441/ceem.15.081. eCollection 2016 Sep.
Red cell distribution width (RDW) is associated with mortality in patients with community-acquired pneumonia (CAP). However, little is known about the effect of changes in RDW during treatment on mortality. Thus, the objective of this study was to evaluate the association between RDW changes and mortality in hospitalized patients with CAP.
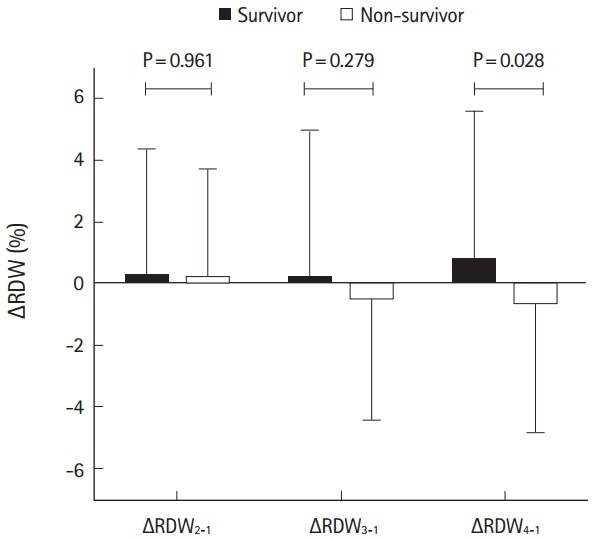
Retrospective analyses were performed using medical records of patients hospitalized for CAP from April 2008 to February 2014. The abstracted laboratory values included RDW (from days one to four), clinical variables, and pneumonia severity index (PSI) scores. The ΔRDW was defined as the change in RDW calculated as: (RDW-RDW)/RDW×100 (%), where 'day n' refers to hospital day.
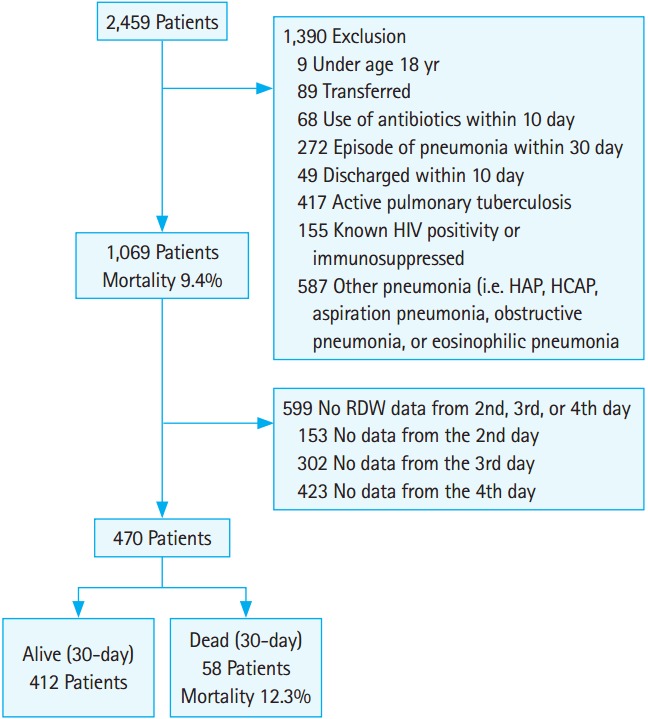
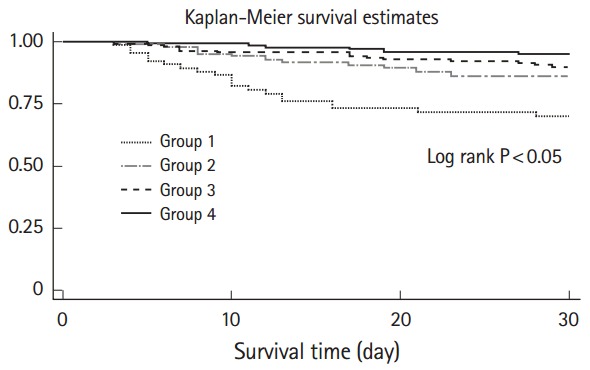
During the study period, a total of 1,069 patients were hospitalized for CAP. The 30-day mortality was 100/1,069 (9.4%). The median RDW at baseline was 14.1% (range, 11.1 to 30.2) and differed significantly between survivors and non-survivors (P<0.05). There were 470 patients with available serial RDW data (30-day mortality 58/470 [12.3%]). Of those, age, PSI score, blood urea nitrogen level, total protein concentration, albumin level, RDW at day 1, and the ΔRDW differed significantly between survivors and non-survivors. Multivariate Cox regression analysis showed that the significance of the relationship between ΔRDW and 30-day mortality risk remained after adjusting for age, PSI score, RDW at day 1, total protein concentration, and initial albumin level.
RDW change from day 1 to day 4 was an independent predictor of mortality in patients with CAP.
红细胞分布宽度(RDW)与社区获得性肺炎(CAP)患者的死亡率相关。然而,关于治疗期间RDW变化对死亡率的影响知之甚少。因此,本研究的目的是评估住院CAP患者RDW变化与死亡率之间的关联。
对2008年4月至2014年2月因CAP住院的患者病历进行回顾性分析。提取的实验室值包括RDW(第1天至第4天)、临床变量和肺炎严重程度指数(PSI)评分。ΔRDW定义为RDW的变化,计算方法为:(RDW - RDW)/RDW×100(%),其中“第n天”指住院日。
在研究期间,共有1069例患者因CAP住院。其30天死亡率为100/1069(9.4%)。基线时RDW的中位数为14.1%(范围为11.1至30.2),幸存者与非幸存者之间存在显著差异(P<0.05)。有470例患者有可用的连续RDW数据(30天死亡率为58/470[12.3%])。其中,幸存者与非幸存者在年龄、PSI评分、血尿素氮水平、总蛋白浓度、白蛋白水平、第1天的RDW和ΔRDW方面存在显著差异。多因素Cox回归分析显示,在调整年龄、PSI评分、第1天的RDW、总蛋白浓度和初始白蛋白水平后,ΔRDW与30天死亡风险之间关系的显著性仍然存在。
第1天至第4天的RDW变化是CAP患者死亡率独立的预测因素。