Zhao Hui, Chen Jing-Yao, Wang Yu-Qian, Lin Zhi-Rong, Wang Shen
Eye Institute of Xiamen University, Xiamen, Fujian 361005; Department of Ophthalmology & Visual Science, Medical College of Xiamen University, Xiamen, Fujian 361005; Fujian Provincial Key Laboratory of Ophthalmology and Visual Science, Xiamen, Fujian 361005; Department of Corneal & Ocular Surface Diseases, Xiamen University Affiliated Xiamen Eye Center, Xiamen, Fujian 361005, China.
Chin Med J (Engl). 2016 Nov 5;129(21):2617-2622. doi: 10.4103/0366-6999.192782.
Dry eye patients suffer from all kinds of symptoms. Sometimes, the clinical signs evaluation does not disclose any obvious difference in routine examination; in vivo confocal microscopy (IVCM) is a powerful tool for ocular surface disease. This study aimed to clarify meibomian gland (MG) alterations in dry eye patients with different symptoms and to compare the findings using IVCM.
A total of sixty patients were recruited, all subjected to Ocular Surface Disease Index (OSDI) and Salisbury Eye Evaluation Questionnaire (SEEQ), and questionnaires for the assessment of dry eye symptoms before clinical sign examinations were given to the patients. Finally, IVCM was applied to observe MG's structure. Statistical analysis was performed using the t-test, Mann-Whitney U-test and Spearman correlation analysis. The differences were statistically significant when P< 0.05.
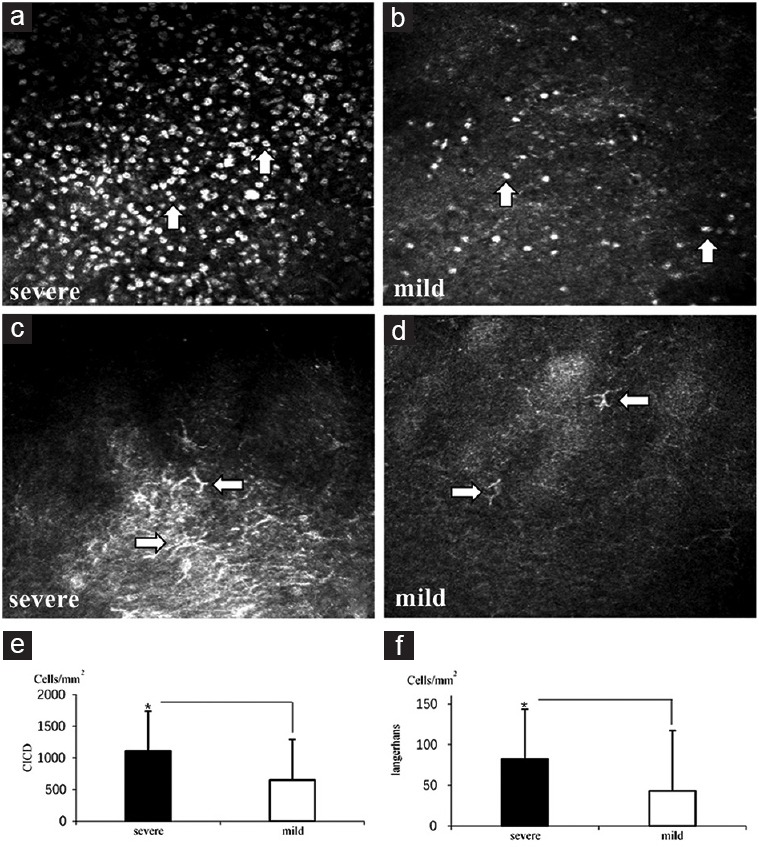
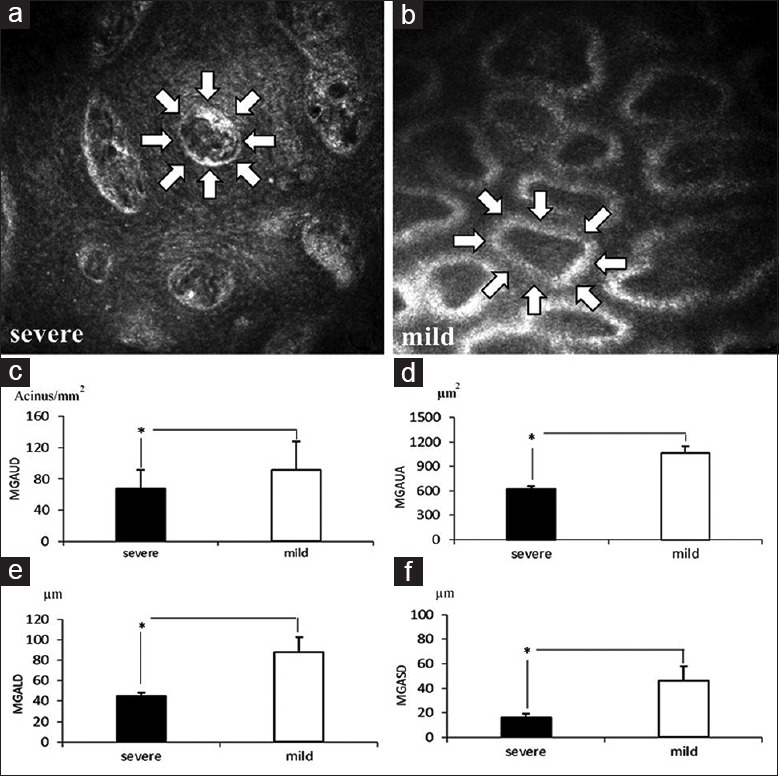
In the severe symptom group, OSDI and SEEQ scores were significantly higher (P< 0.05) compared with the mild symptoms group. All other clinical sign examinations had no statistical difference in the two groups (P> 0.05). However, all the IVCM-observed data showed that patients with severe symptoms had more significant fibrosis in MG (acinar unit area 691.87 ± 182.01 μm2 for the severe, 992.17 ± 170.84 μm2 for the mild; P< 0.05) and severer decrease in the size of MG acinar units than those observed in patients with mild symptoms (MG acinar unit density [MGAUD] 70.08 ± 18.78 glands/mm2, MG acinar unit longest diameter [MGALD] 51.50 ± 15.51 μm, MG acinar unit shortest diameter [MGASD] 20.30 ± 11.85 μm for the severe, MGAUD 89.53 ± 39.88 glands/mm2, MGALD 81.57 ± 21.14 μm, MGASD 42.37 ± 14.55 μm for the mild;P< 0.05). Dry eye symptoms were negatively correlated with MG confocal microscopic parameters and positively correlated with conjunctival inflammatory cells and Langerhans cells (P< 0.05).
IVCM application provides a strong support to differentiate dry eye patients with different symptoms: meibomian gland dysfunction (MGD) plays a pivotal role in dry eye aggravation, and using IVCM to observe MG fibrosis, changes in size and density of MG as well as status of inflammation cells can help not only correctly diagnose the type and severity of dry eye, but also possibly prognosticate in routine eye examination in the occurrence of MGD.
干眼症患者会出现各种症状。有时,临床体征评估在常规检查中未发现任何明显差异;共聚焦显微镜检查(IVCM)是诊断眼表疾病的有力工具。本研究旨在明确不同症状的干眼症患者睑板腺(MG)的改变,并使用IVCM比较研究结果。
共招募60例患者,所有患者均接受眼表疾病指数(OSDI)和索尔兹伯里眼评估问卷(SEEQ)评估,并在临床体征检查前向患者发放干眼症症状评估问卷。最后,应用IVCM观察MG的结构。采用t检验、曼-惠特尼U检验和Spearman相关分析进行统计学分析。当P<0.05时,差异具有统计学意义。
与轻度症状组相比,重度症状组的OSDI和SEEQ评分显著更高(P<0.05)。两组间所有其他临床体征检查均无统计学差异(P>0.05)。然而,所有IVCM观察数据均显示,重度症状患者的MG纤维化更明显(重度组腺泡单位面积为691.87±182.01μm²,轻度组为992.17±170.84μm²;P<0.05),且MG腺泡单位大小的减小程度比轻度症状患者更严重(重度组MG腺泡单位密度[MGAUD]为70.08±18.78个腺/mm²,MG腺泡单位最长直径[MGALD]为51.50±15.51μm,MG腺泡单位最短直径[MGASD]为20.30±11.85μm;轻度组MGAUD为89.53±39.88个腺/mm²,MGALD为81.57±21.14μm,MGASD为42.37±14.55μm;P<0.05)。干眼症症状与MG共聚焦显微镜参数呈负相关,与结膜炎症细胞和朗格汉斯细胞呈正相关(P<0.05)。
IVCM的应用为鉴别不同症状的干眼症患者提供了有力支持:睑板腺功能障碍(MGD)在干眼症加重中起关键作用,使用IVCM观察MG纤维化、MG大小和密度变化以及炎症细胞状态不仅有助于正确诊断干眼症的类型和严重程度,还可能在常规眼科检查中对MGD的发生进行预测。