Yadav Pragya D, Patil Deepak Y, Shete Anita M, Kokate Prasad, Goyal Pulkit, Jadhav Santosh, Sinha Sanjeev, Zawar Divya, Sharma Surendra K, Kapil Arti, Sharma D K, Upadhyay Kamlesh J, Mourya Devendra T
National Institute of Virology, 20-A, Dr. Ambedkar Road, Pune, Maharashtra, Pin Code: 411001, India.
Goyal Hospital and Research Center, Jodhpur, Rajasthan, India.
BMC Infect Dis. 2016 Nov 3;16(1):624. doi: 10.1186/s12879-016-1971-7.
Ever since Crimean-Congo hemorrhagic fever [CCHF] discovered in India, several outbreaks of this disease have been recorded in Gujarat State, India. During the year 2011 to 2015 several districts of Gujarat and Rajasthan state (Sirohi) found to be affected with CCHF including the positivity among ticks and livestock. During these years many infected individuals succumbed to this disease; which subsequently led to nosocomial infections. Herein, we report CCHF cases recorded from Rajasthan state during January 2015. This has affected four individuals apparently associated with one suspected CCHF case admitted in a private hospital in Jodhpur, Rajasthan.
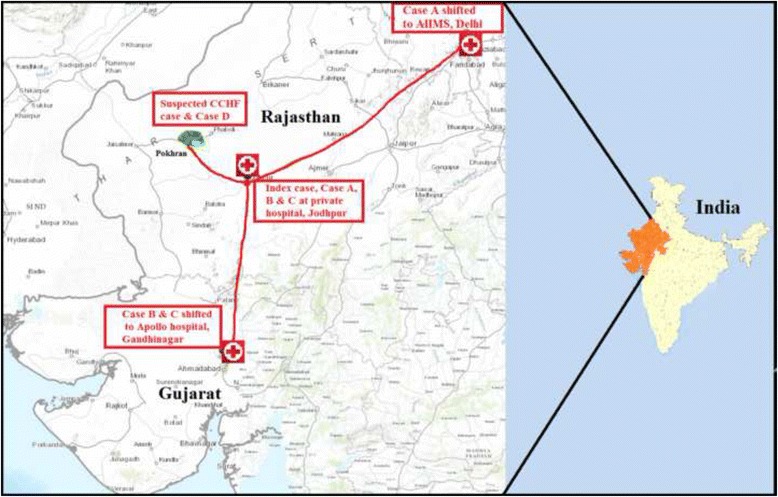
A 30-year-old male was hospitalized in a private hospital in Jodhpur, Rajasthan State, who subsequently had developed thrombocytopenia and showed hemorrhagic manifestations and died in the hospital. Later on, four nursing staff from the same hospital also developed the similar symptoms (Index case and Case A, B, C). Index case succumbed to the disease in the hospital at Jodhpur followed by the death of the case A that was shifted to AIIMS hospital, Delhi due to clinical deterioration. Blood samples of the index case and Case A, B, C were referred to the National institute of Virology, Pune, India for CCHF diagnosis from the different hospitals in Rajasthan, Delhi and Gujarat. However, a sample of deceased suspected CCHF case was not referred. Subsequently, blood samples of 5 nursing staff and 37 contacts (Case D was one of them) from Pokhran area, Jaisalmer district were referred to NIV, Pune.
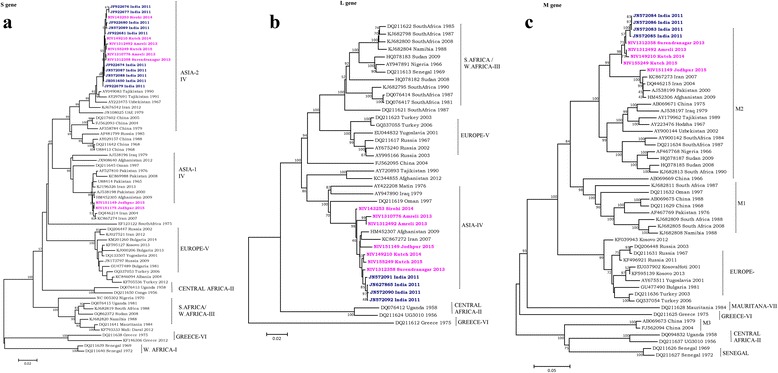
It clearly indicated that nursing staff acquired a nosocomial infection while attending the suspected CCHF case in an Intensive Care Unit of a private hospital in Jodhpur. However, one case was confirmed from the Pokhran area where the suspected CCHF case was residing. This case might have got the infection from suspected CCHF case or through other routes. CCHF strain associated with these nosocomial infections shares the highest identity with Afghanistan strain and its recent introduction from Afghanistan cannot be ruled out. However, lack of active surveillance, unawareness among health care workers leads to such nosocomial infections.
自克里米亚-刚果出血热(CCHF)在印度被发现以来,印度古吉拉特邦已记录了该疾病的数次疫情爆发。在2011年至2015年期间,古吉拉特邦和拉贾斯坦邦(锡罗希)的多个地区被发现受到CCHF影响,包括蜱虫和牲畜中的阳性病例。在这些年里,许多感染者死于这种疾病;随后还导致了医院感染。在此,我们报告2015年1月在拉贾斯坦邦记录的CCHF病例。此次疫情影响了四人,他们显然与拉贾斯坦邦焦特布尔一家私立医院收治的一例疑似CCHF病例有关。
一名30岁男性在拉贾斯坦邦焦特布尔的一家私立医院住院,随后出现血小板减少症并表现出出血症状,最终在医院死亡。后来,同一家医院的四名护理人员也出现了类似症状(索引病例及病例A、B、C)。索引病例在焦特布尔的医院死亡,随后病例A因病情恶化被转至德里的全印医学科学研究所(AIIMS)后死亡。索引病例以及病例A、B、C的血样从拉贾斯坦邦、德里和古吉拉特邦的不同医院被送往印度浦那的国家病毒学研究所进行CCHF诊断。然而,已故疑似CCHF病例的一份样本未被送检。随后,来自斋沙默尔县波克兰地区的5名护理人员和37名接触者(病例D是其中之一)的血样被送往浦那的NIV。
这清楚地表明,护理人员在焦特布尔一家私立医院的重症监护病房护理疑似CCHF病例时获得了医院感染。然而,在疑似CCHF病例居住的波克兰地区确诊了一例病例。该病例可能是从疑似CCHF病例处感染,也可能是通过其他途径感染。与这些医院感染相关的CCHF毒株与阿富汗毒株的同源性最高,不能排除最近从阿富汗传入的可能性。然而,缺乏主动监测以及医护人员意识不足导致了此类医院感染。