Villa Gianluca, Di Maggio Paola, De Gaudio A Raffaele, Novelli Andrea, Antoniotti Riccardo, Fiaccadori Enrico, Adembri Chiara
Department of Health Science, Section of Anesthesiology and Intensive Care, University of Florence, Largo Brambilla 3, Florence, 50134, Italy.
Department of Anesthesia and Intensive Car, Azienda Ospedaliero-Universitaria Careggi, Largo Brambilla 3, Florence, 50134, Italy.
Crit Care. 2016 Nov 19;20(1):374. doi: 10.1186/s13054-016-1551-7.
Major alterations in linezolid pharmacokinetic/pharmacodynamic (PK/PD) parameters might be expected in critically ill septic patients with acute kidney injury (AKI) who are undergoing continuous renal replacement therapy (CRRT). The present review is aimed at describing extracorporeal removal of linezolid and the main PK-PD parameter changes observed in critically ill septic patients with AKI, who are on CRRT.
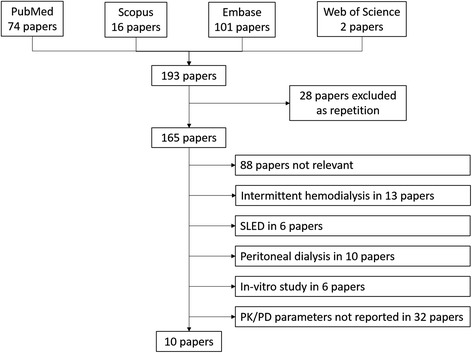
Citations published on PubMed up to January 2016 were systematically reviewed according to the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement. All authors assessed the methodological quality of the studies and consensus was used to ensure studies met inclusion criteria. In-vivo studies in adult patients with AKI treated with linezolid and on CRRT were considered eligible for the analysis only if operational settings of the CRRT machine, membrane type, linezolid blood concentrations and main PK-PD parameters were all clearly reported.
Among 68 potentially relevant articles, only 9 were considered eligible for the analysis. Across these, 53 treatments were identified among the 49 patients included (46 treated with high-flux and 3 with high cut-off membranes). Continuous veno-venous hemofiltration (CVVH) was the most frequent treatment performed amongst the studies. The extracorporeal clearance values of linezolid across the different modalities were 1.2-2.3 L/h for CVVH, 0.9-2.2 L/h for hemodiafiltration and 2.3 L/h for hemodialysis, and large variability in PK/PD parameters was reported. The optimal area under the curve/minimum inhibitory concentration (AUC/MIC) ratio was reached for pathogens with an MIC of 4 mg/L in one study only.
Wide variability in linezolid PK/PD parameters has been observed across critically ill septic patients with AKI treated with CRRT. Particular attention should be paid to linezolid therapy in order to avoid antibiotic failure in these patients. Strategies to improve the effectiveness of this antimicrobial therapy (such as routine use of target drug monitoring, increased posology or extended infusion) should be carefully evaluated, both in clinical and research settings.
对于正在接受持续肾脏替代治疗(CRRT)的急性肾损伤(AKI)重症脓毒症患者,利奈唑胺的药代动力学/药效学(PK/PD)参数可能会发生重大改变。本综述旨在描述利奈唑胺的体外清除情况以及在接受CRRT的AKI重症脓毒症患者中观察到的主要PK-PD参数变化。
根据系统评价和荟萃分析的首选报告项目(PRISMA)声明,对截至2016年1月在PubMed上发表的文献进行系统综述。所有作者评估了研究的方法学质量,并通过达成共识来确保研究符合纳入标准。仅当CRRT机器的操作设置、膜类型、利奈唑胺血药浓度和主要PK-PD参数均明确报告时,才将接受利奈唑胺治疗且正在接受CRRT的成年AKI患者的体内研究纳入分析。
在68篇可能相关的文章中,仅有9篇被认为符合分析条件。在这些文章中,纳入的49例患者共接受了53次治疗(46例采用高通量膜治疗,3例采用高截留膜治疗)。连续性静脉-静脉血液滤过(CVVH)是研究中最常用的治疗方式。不同治疗方式下利奈唑胺的体外清除率分别为:CVVH为1.2 - 2.3 L/h,血液透析滤过为0.9 - 2.2 L/h,血液透析为2.3 L/h,并且报告的PK/PD参数存在很大差异。仅在一项研究中,对于最低抑菌浓度(MIC)为4 mg/L的病原体达到了最佳曲线下面积/最低抑菌浓度(AUC/MIC)比值。
在接受CRRT治疗的AKI重症脓毒症患者中,观察到利奈唑胺的PK/PD参数存在很大差异。应特别关注利奈唑胺治疗,以避免这些患者出现抗生素治疗失败。在临床和研究环境中,都应仔细评估提高这种抗菌治疗效果的策略(如常规使用目标药物监测、增加给药剂量或延长输注时间)。