Hillier-Brown F C, Summerbell C D, Moore H J, Routen A, Lake A A, Adams J, White M, Araujo-Soares V, Abraham C, Adamson A J, Brown T J
Obesity Related Behaviours Research Group, School of Medicine, Pharmacy and Health, Durham University, Stockton-on-Tees, UK.
Fuse - UKCRC Centre for Translational Research in Public Health, Newcastle Upon Tyne, UK.
Obes Rev. 2017 Feb;18(2):227-246. doi: 10.1111/obr.12479. Epub 2016 Nov 29.
Ready-to-eat meals sold by food outlets that are accessible to the general public are an important target for public health intervention. We conducted a systematic review to assess the impact of such interventions.
Studies of any design and duration that included any consumer-level or food-outlet-level before-and-after data were included.
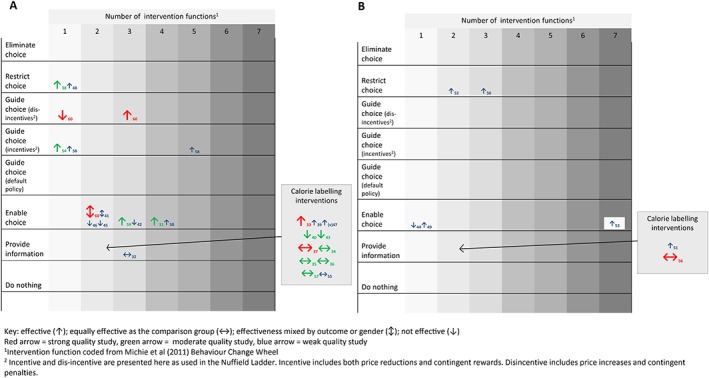
Thirty studies describing 34 interventions were categorized by type and coded against the Nuffield intervention ladder: restrict choice = trans fat law (n = 1), changing pre-packed children's meal content (n = 1) and food outlet award schemes (n = 2); guide choice = price increases for unhealthier choices (n = 1), incentive (contingent reward) (n = 1) and price decreases for healthier choices (n = 2); enable choice = signposting (highlighting healthier/unhealthier options) (n = 10) and telemarketing (offering support for the provision of healthier options to businesses via telephone) (n = 2); and provide information = calorie labelling law (n = 12), voluntary nutrient labelling (n = 1) and personalized receipts (n = 1). Most interventions were aimed at adults in US fast food chains and assessed customer-level outcomes. More 'intrusive' interventions that restricted or guided choice generally showed a positive impact on food-outlet-level and customer-level outcomes. However, interventions that simply provided information or enabled choice had a negligible impact.
Interventions to promote healthier ready-to-eat meals sold by food outlets should restrict choice or guide choice through incentives/disincentives. Public health policies and practice that simply involve providing information are unlikely to be effective.
向公众开放的食品销售点所售即食食品是公共卫生干预的重要目标。我们进行了一项系统综述,以评估此类干预措施的影响。
纳入任何设计和时长、包含任何消费者层面或食品销售点层面前后数据的研究。
30项描述34项干预措施的研究按类型分类,并依据纳菲尔德干预阶梯进行编码:限制选择=反式脂肪法(n=1)、改变儿童预包装食品内容(n=1)以及食品销售点奖励计划(n=2);引导选择=提高不健康食品价格(n=1)、激励(或有奖励)(n=1)以及降低健康食品价格(n=2);便利选择=设置标识(突出更健康/不健康选项)(n=10)以及电话推销(通过电话为企业提供更健康选项提供支持)(n=2);提供信息=卡路里标签法(n=12)、自愿营养标签(n=1)以及个性化收据(n=1)。大多数干预措施针对美国快餐连锁店的成年人,并评估了消费者层面的结果。更多限制或引导选择的“侵入性”干预措施通常对食品销售点层面和消费者层面的结果产生积极影响。然而,单纯提供信息或便利选择的干预措施影响甚微。
促进食品销售点更健康即食食品的干预措施应通过激励/抑制措施来限制选择或引导选择。仅仅涉及提供信息的公共卫生政策和实践不太可能有效。