Kim Taeho, Reardon Kelli, Trifiletti Daniel M, Geesey Constance, Sukovich Kaitlyn, Crandley Edwin, Read Paul W, Wijesooriya Krishni
Virginia Commonwealth University; Virginia Commonwealth University.
J Appl Clin Med Phys. 2016 Nov 8;17(6):60-68. doi: 10.1120/jacmp.v17i6.6324.
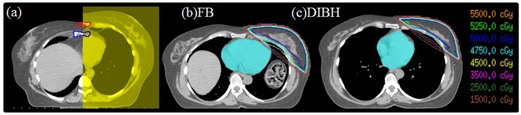
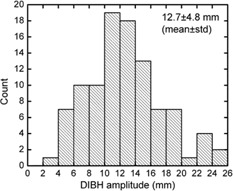
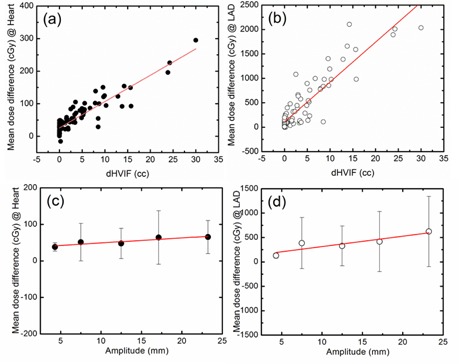
Cardiac irradiation increases the risk of coronary artery disease in patients with left-sided breast cancer. Techniques exist to reduce cardiac irradiation, but the optimum technique depends on individual patient anatomy and physiology. We investigated the correlation of delta heart volume in field (dHVIF) and sternal excursion with dose sparing in heart and left anterior descending artery (LAD) to develop quantitative predictive models for expected dose to heart and LAD. A treatment planning study was performed on 97 left-breast cancer patients who underwent whole breast radiotherapy (prescription dose = 50 Gy) under deep inspiratory breath hold (DIBH). Two CT datasets, free breathing (FB) and DIBH, were utilized for treatment planning and for determination of the internal anatomy-based DIBH amplitude. The mean heart and LAD dose were compared between FB and DIBH plans and dose to the heart and LAD as a function of dHVIF and sternal excursion were determined. The [Average (STD); Range] mean heart doses from free breathing and DIBH are [120.5(65.2); 28.9 ~ 393.8] cGy and [67.5(25.1); 19.7 ~ 145.6] cGy, respectively. The mean LAD doses from free breathing and DIBH are [571.0(582.2); 42.2 ~ 2332.2] cGy and [185.9(127.0); 41.2 ~ 898.4] cGy, respectively. The mean dose reductions with DIBH are [53.1(50.6); -15.4 ~ 295.1] cGy for the heart and [385.1(513.4); -0.6 ~ 2105.8] cGy for LAD. Percent mean dose reductions to the heart and LAD with DIBH are 44% (p < 0.0001) and 67% (p < 0.0001), respectively, compared to FB. The dHVIF mean dose reduction correlation is 8.1 cGy/cc for the heart and 81.6 cGy/cc for LAD (with linear trend and y intercept: 26.0 cGy for the heart, 109.1 cGy for LAD). DIBH amplitude using sternal position was [1.3(.48); .38 ~ 2.5] cm. The DIBH amplitude mean dose reduction correlation is 14 cGy/cm for the heart and 212cGy/cm for LAD (with linear trend with y intercept: 35.6 cGy for the heart, 102.4 cGy for LAD). The strong correlation of dose sparing to the heart and LAD with dHVIF and sternal excursion suggests that mean dose sparing to heart and LAD can be predicted with either dHVIF or sternal excursion equally well. The metrics proposed could be utilized to allow providers to determine the relative dosimetric benefits of different heart-sparing techniques as early as time of consultation.
心脏照射会增加左侧乳腺癌患者患冠状动脉疾病的风险。现有减少心脏照射的技术,但最佳技术取决于个体患者的解剖结构和生理状况。我们研究了野内心脏体积变化量(dHVIF)和胸骨偏移与心脏和左前降支动脉(LAD)剂量 sparing 的相关性,以建立心脏和 LAD 预期剂量的定量预测模型。对 97 例接受全乳放疗(处方剂量 = 50 Gy)且处于深吸气屏气(DIBH)状态的左侧乳腺癌患者进行了一项治疗计划研究。利用两个 CT 数据集,即自由呼吸(FB)和 DIBH 数据集进行治疗计划制定,并确定基于内部解剖结构的 DIBH 幅度。比较了 FB 和 DIBH 计划之间的平均心脏和 LAD 剂量,并确定了心脏和 LAD 剂量与 dHVIF 和胸骨偏移的函数关系。自由呼吸和 DIBH 状态下的[平均(标准差);范围]平均心脏剂量分别为[120.5(65.2);28.9~393.8] cGy 和[67.5(25.1);19.7~145.6] cGy。自由呼吸和 DIBH 状态下的平均 LAD 剂量分别为[571.0(582.2);42.2~2332.2] cGy 和[185.9(127.0);41.2~898.4] cGy。DIBH 状态下心脏的平均剂量减少量为[53.1(50.6);-15.4~295.1] cGy,LAD 的平均剂量减少量为[385.1(513.4);-0.6~2105.8] cGy。与 FB 相比,DIBH 状态下心脏和 LAD 的平均剂量减少百分比分别为 44%(p < 0.0001)和 67%(p < 0.0001)。心脏的 dHVIF 平均剂量减少相关性为 8.1 cGy/cc,LAD 为 81.6 cGy/cc(呈线性趋势,心脏的 y 轴截距为 26.0 cGy,LAD 为 109.1 cGy)。使用胸骨位置的 DIBH 幅度为[1.3(.48);.38~2.5] cm。心脏的 DIBH 幅度平均剂量减少相关性为 14 cGy/cm,LAD 为 21 cGy/cm(呈线性趋势,心脏的 y 轴截距为 35.6 cGy,LAD 为 102.4 cGy)。心脏和 LAD 剂量 sparing 与 dHVIF 和胸骨偏移的强相关性表明,使用 dHVIF 或胸骨偏移同样可以很好地预测心脏和 LAD 的平均剂量 sparing。所提出的指标可用于让医疗服务提供者早在咨询时就能确定不同心脏保护技术的相对剂量学益处。