Yeh Jun-Jun, Wang Yu-Chiao, Lin Che-Chen, Lin Cheng-Li, Hsu Wu-Huei
Ditmanson Medical Foundation Chia-Yi Christian Hospital, Chiayi, Taiwan.
Chia Nan University of Pharmacy and Science, Tainan, Taiwan.
PLoS One. 2016 Dec 22;11(12):e0168673. doi: 10.1371/journal.pone.0168673. eCollection 2016.
The relationship between respiratory tuberculosis (RT) and incident fragility fracture and osteoporosis/fragility fracture in the general population is not well determined; therefore, we conducted a nationwide cohort study to investigate this relationship.
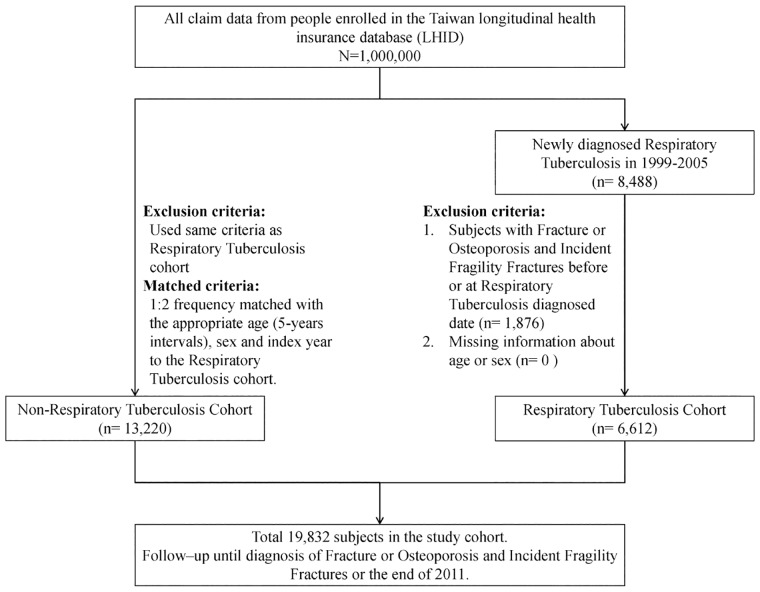
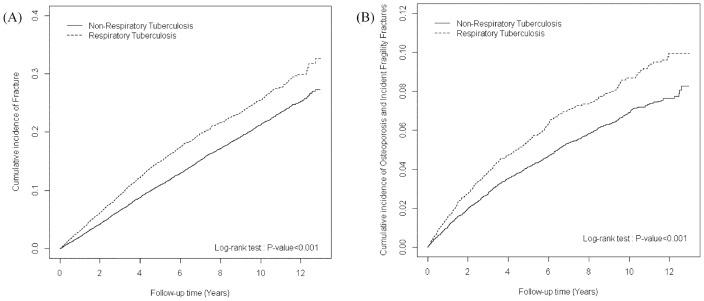
We used the National Health Insurance Research Database of Taiwan to identify 6612 newly diagnosed patients with RT (RT cohort) and 13220 patients without RT (non-RT cohort) from 1999 to 2005. The mean durations of follow-up were (6.73 ± 4.00 years, 8.11 ± 3.24 years) in the (RT cohort, non- RT cohort); respectively. The occurrence of incident fragility fracture and osteoporosis/fragility fracture were followed up until the end of 2011. The adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) and 98% CIs of incident fragility fracture and osteoporosis/fragility fracture were estimated using the multivariable Cox proportional hazard model after adjusting for age, sex, occupation, drug use, and comorbidities.
A Cox proportional hazards regression analysis was performed and showed the aHRs of [incident fragility fracture; osteoporosis/fragility fracture] were [1.69 (95% CI = 1.26-2.28, 98% CI = 1.18-2.44); 1.42 (95% CI = 1.25-1.61, 98% CI = 1.21-1.65)] between the RT and non-RT cohorts. Regarding the sex, the aHRs of the [incident fragility fracture; osteoporosis / fragility fracture] were [1.57 (98% CI = 1.10-2.23, 98% CI = 1.02-2.41); 1.15 (95% CI = 0.97-1.36, 98% CI = 0.94-1.41)] in the men. The aHRs of the RT cohort without oral steroid use in the [incident fragility fracture; osteoporosis / fragility fracture] were [1.87 (95% CI = 1.20-2.90, 98% CI = 1.09-3.19); 1.41 (95% CI = 1.19-1.67, 98% CI = 1.14-1.74)].
The RT associated with the incident fragility fracture, either in men or absence of oral steroid use.
在普通人群中,呼吸道结核病(RT)与新发脆性骨折以及骨质疏松症/脆性骨折之间的关系尚未明确;因此,我们开展了一项全国性队列研究来调查这种关系。
我们利用台湾地区国民健康保险研究数据库,从1999年至2005年中确定了6612例新诊断的RT患者(RT队列)和13220例无RT患者(非RT队列)。(RT队列、非RT队列)的平均随访时间分别为(6.73±4.00年,8.11±3.24年)。对新发脆性骨折和骨质疏松症/脆性骨折的发生情况进行随访直至2011年底。在对年龄、性别、职业、药物使用和合并症进行调整后,使用多变量Cox比例风险模型估计新发脆性骨折和骨质疏松症/脆性骨折的调整后风险比(aHRs)以及95%置信区间(CIs)和98% CIs。
进行了Cox比例风险回归分析,结果显示RT队列与非RT队列之间[新发脆性骨折;骨质疏松症/脆性骨折]的aHRs分别为[1.69(95% CI = 1.26 - 2.28,98% CI = 1.18 - 2.44);1.42(95% CI = 1.25 - 1.61,98% CI = 1.21 - 1.65)]。就性别而言,男性中[新发脆性骨折;骨质疏松症/脆性骨折]的aHRs分别为[1.57(98% CI = 1.10 - 2.23,98% CI = 1.02 - 2.41);1.15(95% CI = 0.97 - 1.36,98% CI = 0.94 - 1.41)]。在未使用口服类固醇的RT队列中,[新发脆性骨折;骨质疏松症/脆性骨折]的aHRs分别为[1.87(95% CI = 1.20 - 2.90,98% CI = 1.09 - 3.19);1.41(95% CI = 1.19 - 1.67,98% CI = 1.14 - 1.74)]。
RT与新发脆性骨折有关,无论男性还是未使用口服类固醇的情况均如此。