Ellingsen Øyvind, Halle Martin, Conraads Viviane, Støylen Asbjørn, Dalen Håvard, Delagardelle Charles, Larsen Alf-Inge, Hole Torstein, Mezzani Alessandro, Van Craenenbroeck Emeline M, Videm Vibeke, Beckers Paul, Christle Jeffrey W, Winzer Ephraim, Mangner Norman, Woitek Felix, Höllriegel Robert, Pressler Axel, Monk-Hansen Tea, Snoer Martin, Feiereisen Patrick, Valborgland Torstein, Kjekshus John, Hambrecht Rainer, Gielen Stephan, Karlsen Trine, Prescott Eva, Linke Axel
From St. Olavs Hospital, Trondheim University Hospital, Norway (Ø.E., A.S., H.D., V.V., T.K.); K.G. Jebsen Center for Exercise in Medicine, Department of Circulation and Medical Imaging, Norwegian University of Science and Technology, Trondheim, Norway (Ø.E., H.D., T.K.); Department of Prevention, Rehabilitation and Sports Medicine, Technische Universität München, Klinikum rechts der Isar, Germany (M.H., J.W.C., A.P.); DZHK (German Center for Cardiovascular Research), Partner Site Munich Heart Alliance, Munich, Germany (M.H.); Else-Kröner-Fresenius Prevention Center, Klinikum rechts der Isar, Munich, Germany (M.H.); Antwerp University Hospital, Edegem, Belgium (V.C., E.M.V.C., P.B.); University of Antwerp, Belgium (V.C., E.M.V.C., P.B.); Department of Circulation and Medical Imaging (A.S., T.H.) and Department of Laboratory Medicine, Children's and Women's Health (V.V.), NTNU-Norwegian University of Science and Technology, Trondheim, Norway; Department of Medicine, Levanger Hospital, Nord-Trøndelag Hospital Trust, Norway (H.D.); Centre Hospitalier de Luxembourg, Luxembourg (C.D., P.F.); Department of Cardiology, Stavanger University Hospital, Norway (A.- I.L., T.V.); Department of Clinical Science, University of Bergen, Norway (A.-I.L., T.V.); Ålesund Hospital, Møre og Romsdal Health Trust, Norway (T.H.); Cardiac Rehabilitation Division, Salvatore Maugeri Foundation IRCCS, Scientific Institute of Veruno, Italy (A.M.); Division of Cardiovascular Medicine, Stanford Center for Inherited Cardiovascular Disease, CA (J.W.C.); Department of Cardiology, Herzzentrum, Universität Leipzig, Germany (E.W., N.M., F.W., R. Höllriegel, A.L.); Department of Cardiology, Bispebjerg Hospital, University of Copenhagen, Denmark (T.M.-H., M.S., E.P.); University of Oslo, Rikshospitalet University Hospital, Norway (J.K.); Department of Cardiology and Angiology, Klinikum Links der Weser, Bremen, Germany (R. Hambrecht); and Department of Cardiology, Angiology and Intensive Care, Klinikum Lippe, Detmold, Germany (S.G.).
Circulation. 2017 Feb 28;135(9):839-849. doi: 10.1161/CIRCULATIONAHA.116.022924. Epub 2017 Jan 12.
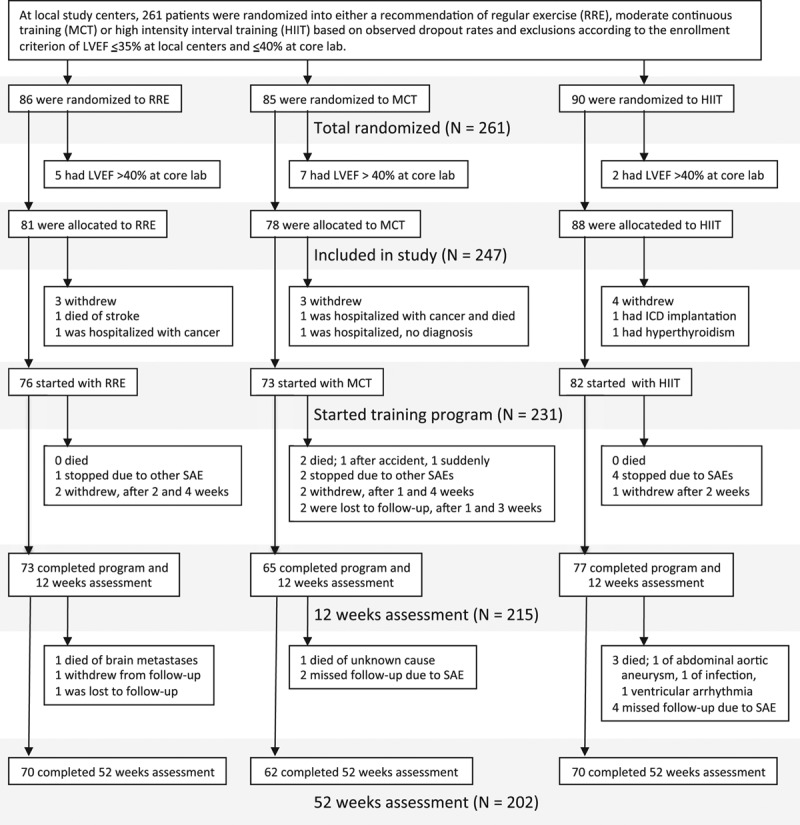
Small studies have suggested that high-intensity interval training (HIIT) is superior to moderate continuous training (MCT) in reversing cardiac remodeling and increasing aerobic capacity in patients with heart failure with reduced ejection fraction. The present multicenter trial compared 12 weeks of supervised interventions of HIIT, MCT, or a recommendation of regular exercise (RRE).
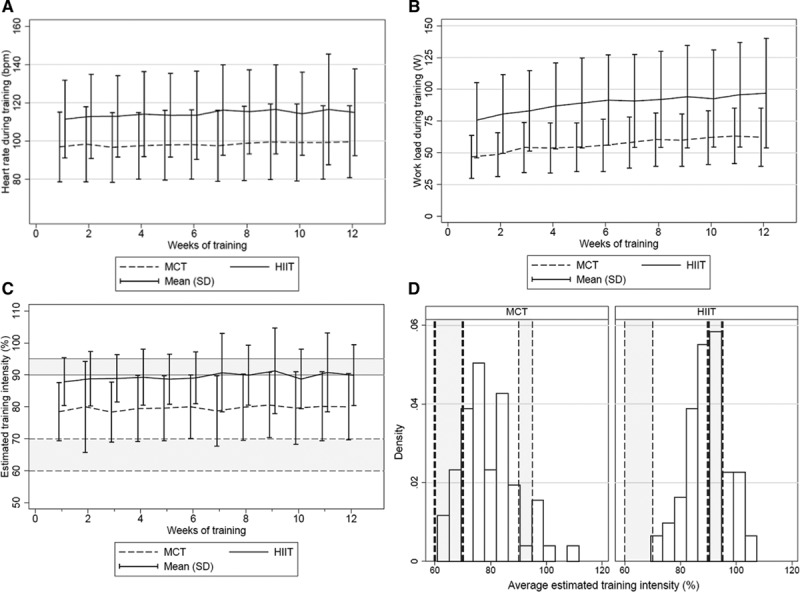
Two hundred sixty-one patients with left ventricular ejection fraction ≤35% and New York Heart Association class II to III were randomly assigned to HIIT at 90% to 95% of maximal heart rate, MCT at 60% to 70% of maximal heart rate, or RRE. Thereafter, patients were encouraged to continue exercising on their own. Clinical assessments were performed at baseline, after the intervention, and at follow-up after 52 weeks. Primary end point was a between-group comparison of change in left ventricular end-diastolic diameter from baseline to 12 weeks.
Groups did not differ in age (median, 60 years), sex (19% women), ischemic pathogenesis (59%), or medication. Change in left ventricular end-diastolic diameter from baseline to 12 weeks was not different between HIIT and MCT (=0.45); left ventricular end-diastolic diameter changes compared with RRE were -2.8 mm (-5.2 to -0.4 mm; =0.02) in HIIT and -1.2 mm (-3.6 to 1.2 mm; =0.34) in MCT. There was also no difference between HIIT and MCT in peak oxygen uptake (=0.70), but both were superior to RRE. However, none of these changes was maintained at follow-up after 52 weeks. Serious adverse events were not statistically different during supervised intervention or at follow-up at 52 weeks (HIIT, 39%; MCT, 25%; RRE, 34%; =0.16). Training records showed that 51% of patients exercised below prescribed target during supervised HIIT and 80% above target in MCT.
HIIT was not superior to MCT in changing left ventricular remodeling or aerobic capacity, and its feasibility remains unresolved in patients with heart failure.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT00917046.
小型研究表明,在射血分数降低的心力衰竭患者中,高强度间歇训练(HIIT)在逆转心脏重塑和提高有氧能力方面优于中等强度持续训练(MCT)。本多中心试验比较了12周的HIIT、MCT监督干预或常规运动建议(RRE)。
261例左心室射血分数≤35%且纽约心脏协会心功能分级为II至III级的患者被随机分配至最大心率90%至95%的HIIT组、最大心率60%至70%的MCT组或RRE组。此后,鼓励患者自行继续锻炼。在基线、干预后以及52周随访时进行临床评估。主要终点是组间比较从基线到12周左心室舒张末期直径的变化。
各组在年龄(中位数60岁)、性别(19%为女性)、缺血性发病机制(59%)或药物治疗方面无差异。HIIT组和MCT组从基线到12周左心室舒张末期直径的变化无差异(P = 0.45);与RRE组相比,HIIT组左心室舒张末期直径变化为-2.8 mm(-5.2至-0.4 mm;P = 0.02),MCT组为-1.2 mm(-3.6至1.2 mm;P = 0.34)。HIIT组和MCT组在峰值摄氧量方面也无差异(P = 0.70),但两者均优于RRE组。然而,52周随访时这些变化均未维持。在监督干预期间或52周随访时,严重不良事件在统计学上无差异(HIIT组39%;MCT组25%;RRE组34%;P = 0.16)。训练记录显示,51%的患者在监督的HIIT期间运动强度低于规定目标,80%的患者在MCT期间运动强度高于目标。
HIIT在改变左心室重塑或有氧能力方面并不优于MCT,其在心力衰竭患者中的可行性仍未解决。