Broeg-Morvay Anne, Mordasini Pasquale, Slezak Agnieszka, Liesirova Kai, Meisterernst Julia, Schroth Gerhard, Arnold Marcel, Jung Simon, Mattle Heinrich P, Gralla Jan, Fischer Urs
Department of Neurology, Inselspital, University Hospital Bern and University of Bern, Bern, Switzerland.
Department of Diagnostic and Interventional Neuroradiology, Inselspital, University Hospital Bern and University of Bern, Bern, Switzerland.
PLoS One. 2017 Jan 17;12(1):e0170045. doi: 10.1371/journal.pone.0170045. eCollection 2017.
Symptomatic intracerebral hemorrhage (sICH) after bridging thrombolysis for acute ischemic stroke is a devastating complication. We aimed to assess whether the additional administration of aspirin during endovascular intervention increases bleeding rates.
We retrospectively compared bleeding complications and outcome in stroke patients who received bridging thrombolysis with (tPA+ASA) and without (tPA-ASA) aspirin during endovascular intervention between November 2008 and March 2014. Furthermore, we analyzed bleeding complications and outcome in antiplatelet naïve patients with those with prior or acute antiplatelet therapy.
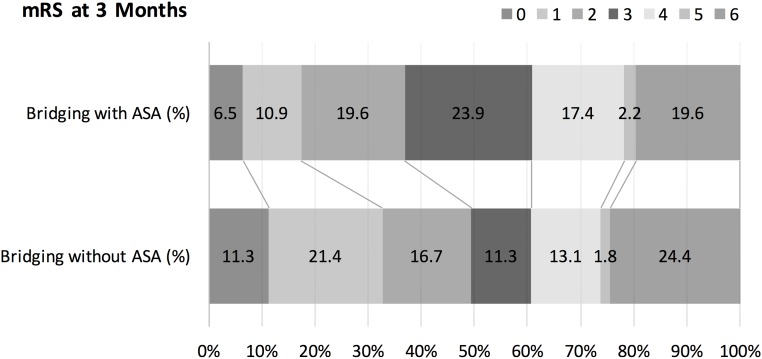
Baseline characteristics, previous medication, and dosage of rtPA did not differ between 50 tPA+ASA (39 aspirin naïve, 11 preloaded) and 181 tPA-ASA patients (p>0.05). tPA+ASA patients had more often internal carotid artery (ICA) occlusion (p<0.001), large artery disease (p<0.001) and received more often acute stenting of the ICA (p<0.001). 10/180 (5.6%) tPA-ASA patients and 3/49 (6.1%) tPA+ASA patients suffered a sICH (p = 1.0). Rates of asymptomatic intracerebral hemorrhage, systemic bleeding complications and outcome did not differ between both groups (p>0.1). There were no differences in bleeding complications and mortality among 112 bridging patients with antiplatelet therapy (62 preloaded, 39 acute administration, 11 both) and 117 antiplatelet naïve patients. In a logistic regression analysis, aspirin administration during endovascular procedure was not a predictor of sICH.
Antiplatelet therapy before or during bridging thrombolysis in patients with acute ischemic stroke did not increase the risk of bleeding complications and had no impact on outcome. This finding has to be confirmed in larger studies.
急性缺血性卒中桥接溶栓后出现的症状性脑出血(sICH)是一种严重的并发症。我们旨在评估血管内介入治疗期间额外给予阿司匹林是否会增加出血率。
我们回顾性比较了2008年11月至2014年3月期间在血管内介入治疗期间接受桥接溶栓并服用阿司匹林(tPA + ASA)和未服用阿司匹林(tPA - ASA)的卒中患者的出血并发症及预后情况。此外,我们分析了未接受过抗血小板治疗的患者与接受过抗血小板治疗或急性抗血小板治疗的患者的出血并发症及预后情况。
50例tPA + ASA患者(39例未服用过阿司匹林,11例预先服用过)和181例tPA - ASA患者之间的基线特征、既往用药情况及rtPA剂量无差异(p>0.05)。tPA + ASA组患者颈内动脉(ICA)闭塞、大动脉疾病更为常见(p<0.001),且更常接受ICA急性支架置入术(p<0.001)。180例tPA - ASA患者中有10例(5.6%)发生sICH,49例tPA + ASA患者中有3例(6.1%)发生sICH(p = 1.0)。两组间无症状性脑出血、全身性出血并发症及预后情况无差异(p>0.1)。112例接受抗血小板治疗的桥接患者(62例预先服用,39例急性给药,11例两者皆有)和117例未接受抗血小板治疗的患者在出血并发症及死亡率方面无差异。在逻辑回归分析中,血管内手术期间给予阿司匹林并非sICH的预测因素。
急性缺血性卒中患者在桥接溶栓前或期间进行抗血小板治疗不会增加出血并发症风险,且对预后无影响。这一发现有待更大规模研究证实。