Huiskes Victor Johan Bernard, Burger David Marinus, van den Ende Cornelia Helena Maria, van den Bemt Bartholomeus Johannes Fredericus
Department of Pharmacy, Sint Maartenskliniek, Hengstdal 3, 6574 NA, Ubbergen, The Netherlands.
Department of Pharmacy, Radboud University Medical Center, Geert Grooteplein-Zuid 10, 6525 GA, Nijmegen, The Netherlands.
BMC Fam Pract. 2017 Jan 17;18(1):5. doi: 10.1186/s12875-016-0577-x.
Medication review is often recommended to optimize medication use. In clinical practice it is mostly operationalized as an intervention without co-interventions during a short term intervention period. However, most systematic reviews also included co-interventions and prolonged medication optimization interventions. Furthermore, most systematic reviews focused on specific patient groups (e.g. polypharmacy, elderly, hospitalized) and/or on specific outcome measures (e.g. hospital admissions and mortality). Therefore, the objective of this study is to assess the effectiveness of medication review as an isolated short-term intervention, irrespective of the patient population and the outcome measures used.
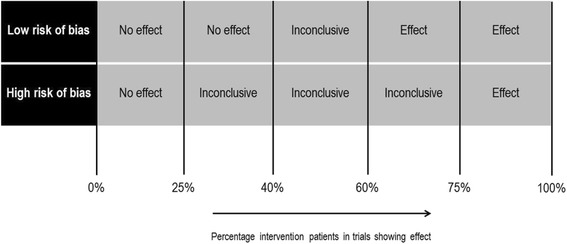
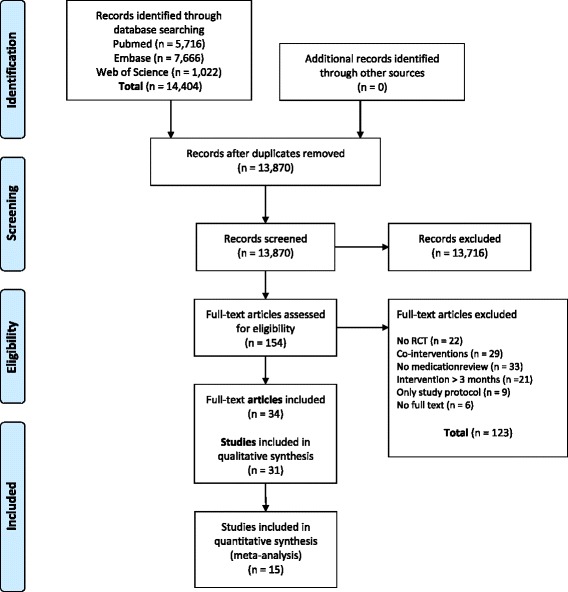
A literature search was performed in MEDLINE, EMBASE and Web of Science from their inception through September 2015. Randomized controlled trials (RCTs) with medication review as isolated short term intervention (<3 months) were included. There were no restrictions with regard to patient characteristics and outcome measures. One reviewer extracted and a second checked data. The risk of bias of studies was evaluated independently by two reviewers. A best evidence synthesis was conducted for every outcome measure used in more than one trial. In case of binary variables a meta-analysis was performed in addition to the best evidence synthesis, to quantify the effect.
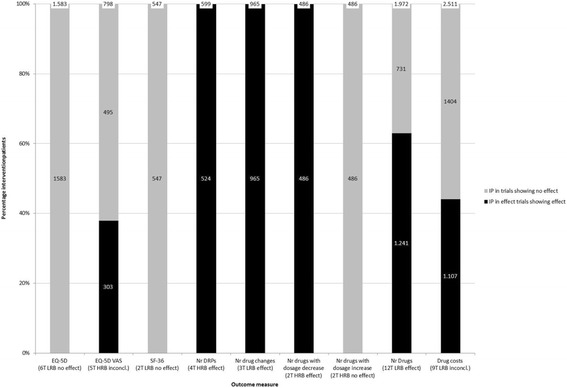
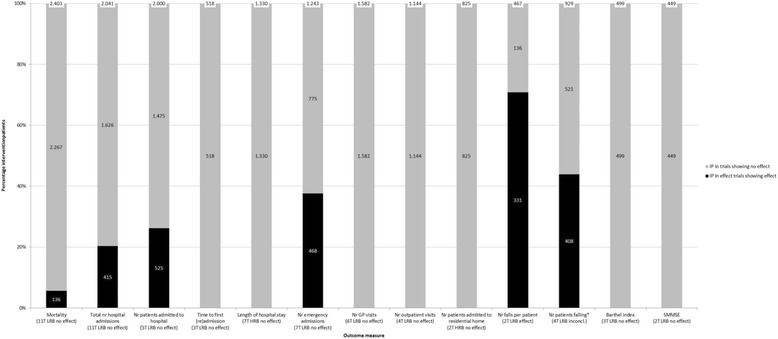
Thirty-one RCTs were included in this systematic review (55% low risk of bias). A best evidence synthesis was conducted for 22 outcome measures. No effect of medication review was found on clinical outcomes (mortality, hospital admissions/healthcare use, the number of patients falling, physical and cognitive functioning), except a decrease in the number of falls per patient. However, in a sensitivity analysis using a more stringent threshold for risk of bias, the conclusion for the effect on the number of falls changed to inconclusive. Furthermore no effect was found on quality of life and evidence was inconclusive about the effect on economical outcome measures. However, an effect was found on most drug-related problems: medication review resulted in a decrease in the number of drug-related problems, more changes in medication, more drugs with dosage decrease and a greater decrease or smaller increase of the number of drugs.
An isolated medication review during a short term intervention period has an effect on most drug-related outcomes, minimal effect on clinical outcomes and no effect on quality of life. No conclusion can be drawn about the effect on economical outcome measures. Therefore, it should be considered to stop performing cross-sectional medication reviews as standard care.
药物评估常被推荐用于优化药物使用。在临床实践中,它大多作为一种在短期干预期间无联合干预措施的干预手段来实施。然而,大多数系统评价也纳入了联合干预措施以及延长的药物优化干预措施。此外,大多数系统评价聚焦于特定患者群体(如多重用药、老年人、住院患者)和/或特定结局指标(如住院和死亡率)。因此,本研究的目的是评估药物评估作为一种单独的短期干预措施的有效性,而不考虑患者群体和所使用的结局指标。
在MEDLINE、EMBASE和Web of Science数据库中进行了从建库至2015年9月的文献检索。纳入以药物评估作为单独短期干预措施(<3个月)的随机对照试验(RCT)。对患者特征和结局指标没有限制。由一名审阅者提取数据,另一名进行核对。两名审阅者独立评估研究的偏倚风险。对在一项以上试验中使用的每个结局指标进行最佳证据综合分析。对于二元变量,除了最佳证据综合分析外,还进行了荟萃分析以量化效应。
本系统评价纳入了31项RCT(55%为低偏倚风险)。对22个结局指标进行了最佳证据综合分析。未发现药物评估对临床结局(死亡率、住院/医疗保健使用、跌倒患者数量、身体和认知功能)有影响,但每位患者的跌倒次数有所减少。然而,在一项使用更严格偏倚风险阈值的敏感性分析中,关于对跌倒次数影响的结论变为不确定。此外,未发现对生活质量有影响,关于对经济结局指标的影响证据也不确定。然而,发现对大多数药物相关问题有影响:药物评估导致药物相关问题数量减少、用药变化更多、剂量减少的药物更多,以及药物数量减少幅度更大或增加幅度更小。
在短期干预期间单独进行药物评估对大多数药物相关结局有影响,对临床结局影响极小,对生活质量无影响。关于对经济结局指标的影响无法得出结论。因此,应考虑停止将横断面药物评估作为标准治疗方法。