Hu Peter T, Lopes Renato D, Stevens Susanna R, Wallentin Lars, Thomas Laine, Alexander John H, Hanna Michael, Lewis Basil S, Verheugt Freek W A, Granger Christopher B, Jones W Schuyler
Department of Medicine, Duke University Medical Center, Durham, NC.
Duke Clinical Research Institute, Duke University Medical Center, Durham, NC.
J Am Heart Assoc. 2017 Jan 17;6(1):e004699. doi: 10.1161/JAHA.116.004699.
We studied (1) the rates of stroke or systemic embolism and bleeding in patients with atrial fibrillation and peripheral artery disease (PAD) and (2) the efficacy and safety of apixaban versus warfarin in patients with atrial fibrillation with and without PAD.
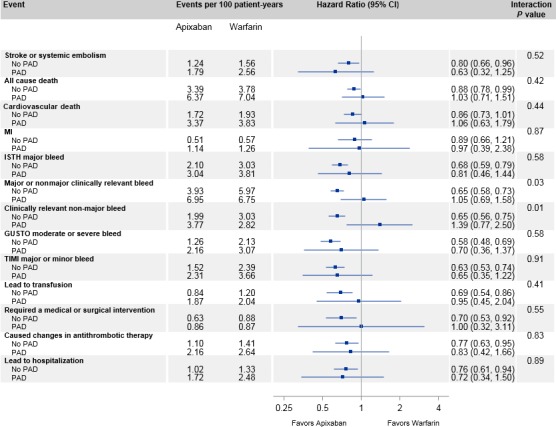
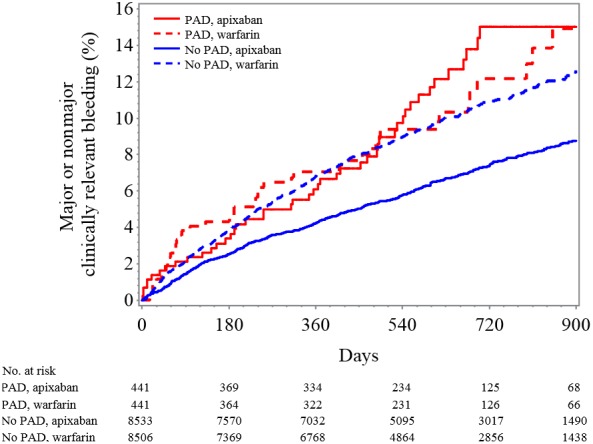
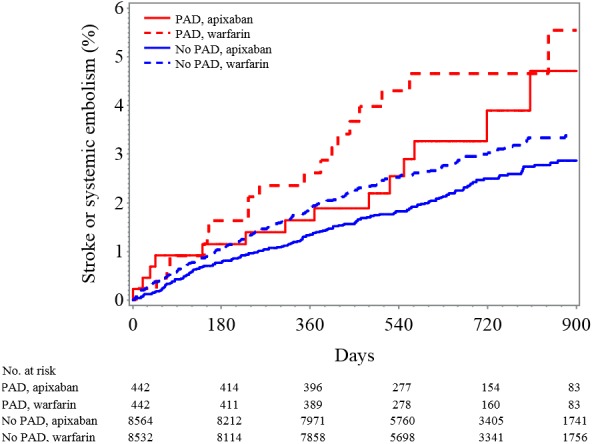
The Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial randomized 18 201 patients with atrial fibrillation to apixaban or warfarin for stroke/systemic embolism prevention; 884 (4.9%) patients had PAD at baseline. Patients with PAD had higher unadjusted rates of stroke and systemic embolism (hazard ratio [HR] 1.73, 95% CI 1.22-2.45; P=0.002) and major bleeding (HR 1.34, 95% CI 1.00-1.81; P=0.05), but after adjustment, no differences existed in rates of stroke and systemic embolism (HR 1.32, 95% CI 0.93-1.88; P=0.12) and major bleeding (HR 1.03, 95% CI 0.76-1.40; P=0.83) compared with patients without PAD. The risk of stroke or systemic embolism was similar in patients assigned to apixaban and warfarin with PAD (HR 0.63, 95% CI 0.32-1.25) and without PAD (HR 0.80, 95% CI 0.66-0.96; interaction P=0.52). Patients with PAD did not have a statistically significant reduction in major or clinically relevant nonmajor bleeding with apixaban compared with warfarin (HR 1.05, 95% CI 0.69-1.58), whereas those without PAD had a statistically significant reduction (HR 0.65, 95% CI 0.58-0.73; interaction P=0.03).
Patients with PAD in ARISTOTLE had a higher crude risk of stroke or systemic embolism compared with patients without PAD that was not present after adjustment. The benefits of apixaban versus warfarin for stroke and systemic embolism were similar in patients with and without PAD. These findings highlight the need to optimize the treatment of patients with atrial fibrillation and PAD.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT00412984.
我们研究了(1)心房颤动合并外周动脉疾病(PAD)患者的中风或全身性栓塞及出血发生率,以及(2)阿哌沙班与华法林在合并和不合并PAD的心房颤动患者中的疗效和安全性。
心房颤动减少中风及其他血栓栓塞事件(ARISTOTLE)试验将18201例心房颤动患者随机分为阿哌沙班组或华法林组以预防中风/全身性栓塞;884例(4.9%)患者基线时有PAD。有PAD的患者未经调整的中风和全身性栓塞发生率较高(风险比[HR]1.73,95%置信区间1.22 - 2.45;P = 0.002)以及大出血发生率较高(HR 1.34,95%置信区间1.00 - 1.81;P = 0.05),但调整后,与无PAD的患者相比,中风和全身性栓塞发生率(HR 1.32,95%置信区间0.93 - 1.88;P = 0.12)以及大出血发生率(HR 1.03,95%置信区间0.76 - 1.40;P = 0.83)无差异。在有PAD的患者中,分配至阿哌沙班组和华法林组的患者中风或全身性栓塞风险相似(HR 0.63,95%置信区间0.32 - 1.25),在无PAD的患者中也相似(HR 0.80,95%置信区间0.66 - 0.96;交互作用P = 0.52)。与华法林相比,有PAD的患者使用阿哌沙班后大出血或临床相关非大出血的减少无统计学意义(HR 1.05,95%置信区间0.69 - 1.58),而无PAD的患者有统计学意义的减少(HR