Rees Chris A, Flick Robert J, Sullivan David, Bvumbwe Menard, Mhango Joseph, Hosseinipour Mina C, Kazembe Peter N
Baylor College of Medicine Children's Foundation Malawi, Lilongwe, Malawi.
Baylor College of Medicine, Houston, Texas, United States of America.
PLoS One. 2017 Jan 18;12(1):e0169057. doi: 10.1371/journal.pone.0169057. eCollection 2017.
Human immunodeficiency virus (HIV) contributes to nearly 20% of all deaths in children under five years of age in Malawi. Expanded coverage of antiretroviral therapy has allowed children to access treatment on an outpatient basis. Little is known about characteristics of the final outpatient encounter prior to mortality in the outpatient setting.
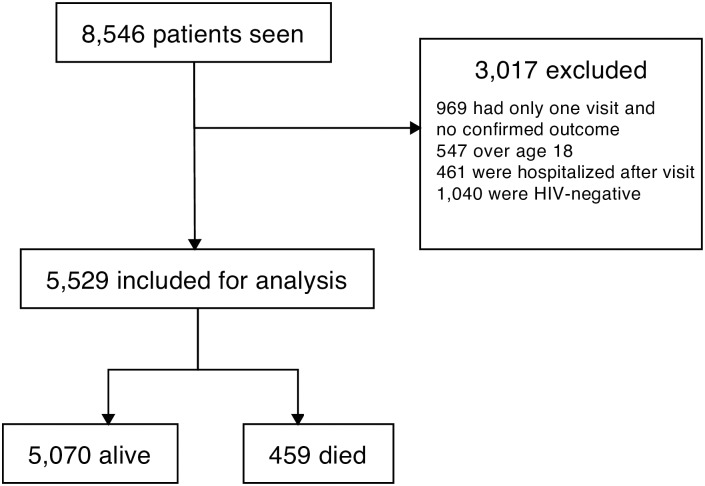
This retrospective cohort study assessed clinical factors associated with mortality among HIV-exposed infants and HIV-infected children less than 18 years of age at the Baylor College of Medicine Abbott Fund Children's Center of Excellence in Lilongwe, Malawi. We compared clinical indicators documented from the final outpatient encounter for patients who died in the outpatient setting versus those who were alive after their penultimate clinical encounter.
Of the 8,546 patients who were attended to over a 10-year period at the Baylor Center of Excellence, 851 had died (10%). Of children who died, 392 (46%) were directly admitted to the hospital after their last clinical encounter and died as inpatients. Of the remaining 459 who died as outpatients after their last visit, 53.5% had a World Health Organization (WHO) stage IV condition at their last visit, and 25% had a WHO stage III condition. Multivariate regression analysis demonstrated that poor nutritional status, female gender, shorter time as a patient, more clinical encounters in the prior month, if last visit was an unscheduled sick visit, and if the patient had lost weight since their prior visit independently predicted increased mortality in the outpatient setting after the final clinical encounter.
Clinical indicators may assist in identifying children with HIV who have increased risk of mortality in the outpatient setting. Recognizing these indicators may aid in identifying HIV-infected children who require a higher level of care or closer follow-up.
在马拉维,人类免疫缺陷病毒(HIV)导致近20%的五岁以下儿童死亡。抗逆转录病毒疗法覆盖面的扩大使儿童能够在门诊接受治疗。对于门诊环境中死亡前最后一次门诊就诊的特征,人们了解甚少。
这项回顾性队列研究评估了马拉维利隆圭贝勒医学院雅培基金卓越儿童中心18岁以下暴露于HIV的婴儿和感染HIV儿童中与死亡相关的临床因素。我们比较了在门诊环境中死亡的患者与倒数第二次临床就诊后仍存活的患者最后一次门诊就诊记录的临床指标。
在卓越贝勒中心10年期间就诊的8546名患者中,851人死亡(10%)。在死亡的儿童中,392人(46%)在最后一次临床就诊后直接住院并作为住院患者死亡。在最后一次就诊后作为门诊患者死亡的其余459人中,53.5%在最后一次就诊时处于世界卫生组织(WHO)IV期,25%处于WHO III期。多变量回归分析表明,营养状况差、女性、患者病程较短、前一个月临床就诊次数较多、最后一次就诊是否为非计划内病假就诊以及自上次就诊后体重是否减轻,均独立预测最后一次临床就诊后门诊环境中死亡率增加。
临床指标可能有助于识别门诊环境中死亡风险增加的HIV感染儿童。识别这些指标可能有助于识别需要更高水平护理或更密切随访的HIV感染儿童。