Schwenkenbecher Philipp, Pul Refik, Wurster Ulrich, Conzen Josef, Pars Kaweh, Hartmann Hans, Sühs Kurt-Wolfram, Sedlacek Ludwig, Stangel Martin, Trebst Corinna, Skripuletz Thomas
Department of Neurology, Hannover Medical School, Carl-Neuberg-Str. 1, 30625, Hannover, Germany.
Department of Diagnostic and Interventional Neuroradiology, Hannover Medical School, Hannover, Germany.
BMC Infect Dis. 2017 Jan 21;17(1):90. doi: 10.1186/s12879-016-2112-z.
Neuroborreliosis represents a relevant infectious disease and can cause a variety of neurological manifestations. Different stages and syndromes are described and atypical symptoms can result in diagnostic delay or misdiagnosis. The aim of this retrospective study was to define the pivotal neurological deficits in patients with neuroborreliosis that were the reason for admission in a hospital.
We retrospectively evaluated data of patients with neuroborreliosis. Only patients who fulfilled the diagnostic criteria of an intrathecal antibody production against Borrelia burgdorferi were included in the study.
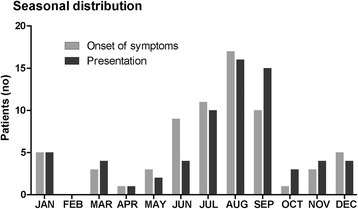
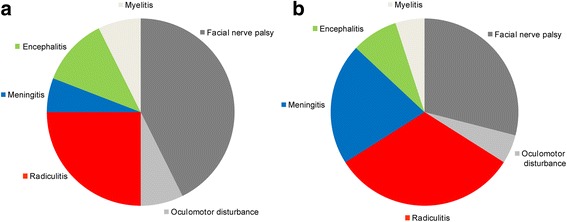
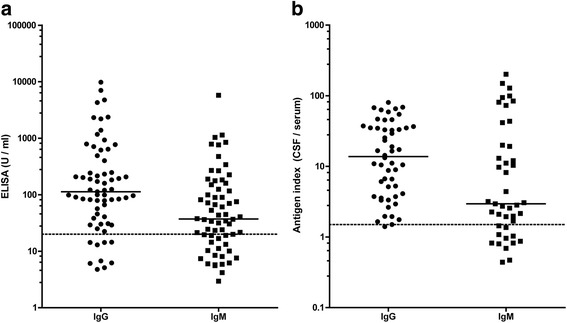
Sixty-eight patients were identified with neuroborreliosis. Cranial nerve palsy was the most frequent deficit (50%) which caused admission to a hospital followed by painful radiculitis (25%), encephalitis (12%), myelitis (7%), and meningitis/headache (6%). In patients with a combination of deficits, back pain was the first symptom, followed by headache, and finally by cranial nerve palsy. Indeed, signs of meningitis were often found in patients with neuroborreliosis, but usually did not cause admission to a hospital. Unusual cases included patients with sudden onset paresis that were initially misdiagnosed as stroke and one patient with acute delirium. Cerebrospinal fluid (CSF) analysis revealed typical changes including elevated CSF cell count in all but one patient, a blood-CSF barrier dysfunction (87%), CSF oligoclonal bands (90%), and quantitative intrathecal synthesis of immunoglobulins (IgM in 74%, IgG in 47%, and IgA in 32% patients). Importantly, 6% of patients did not show Borrelia specific antibodies in the blood.
In conclusion, the majority of patients presented with typical neurological deficits. However, unusual cases such as acute delirium indicate that neuroborreliosis has to be considered in a wide spectrum of neurological diseases. CSF analysis is essential for a reliable diagnosis of neuroborreliosis.
神经莱姆病是一种重要的传染病,可导致多种神经表现。该病有不同的阶段和综合征描述,非典型症状可能导致诊断延迟或误诊。这项回顾性研究的目的是确定神经莱姆病患者导致其入院的关键神经功能缺损。
我们回顾性评估了神经莱姆病患者的数据。本研究仅纳入符合针对伯氏疏螺旋体鞘内抗体产生诊断标准的患者。
共识别出68例神经莱姆病患者。脑神经麻痹是最常见的导致入院的功能缺损(50%),其次是疼痛性神经根炎(25%)、脑炎(12%)、脊髓炎(7%)和脑膜炎/头痛(6%)。在合并多种功能缺损的患者中,背痛是首发症状,其次是头痛,最后是脑神经麻痹。实际上,神经莱姆病患者中常发现脑膜炎体征,但通常不会导致入院。不寻常的病例包括最初被误诊为中风的突发麻痹患者和1例急性谵妄患者。脑脊液(CSF)分析显示典型变化,除1例患者外所有患者的脑脊液细胞计数均升高,血脑屏障功能障碍(87%),脑脊液寡克隆带(90%),以及免疫球蛋白的定量鞘内合成(74%的患者有IgM,47%的患者有IgG,32%的患者有IgA)。重要的是,6%的患者血液中未显示伯氏疏螺旋体特异性抗体。
总之,大多数患者表现为典型的神经功能缺损。然而,急性谵妄等不寻常病例表明,在广泛的神经系统疾病中都必须考虑神经莱姆病。脑脊液分析对于神经莱姆病的可靠诊断至关重要。