Saldanha Maíra G, Queiroz Adriano, Machado Paulo Roberto L, de Carvalho Lucas P, Scott Phillip, de Carvalho Filho Edgar M, Arruda Sérgio
Instituto Gonçalo Moniz, Fundação Oswaldo Cruz (FIOCRUZ), Salvador, Bahia, Brazil.
Serviço de Imunologia, Complexo Hospitalar Universitário Professor Edgard Santos, Universidade Federal da Bahia, Salvador, Bahia, Brazil.
Am J Trop Med Hyg. 2017 Mar;96(3):645-652. doi: 10.4269/ajtmh.16-0539. Epub 2017 Apr 6.
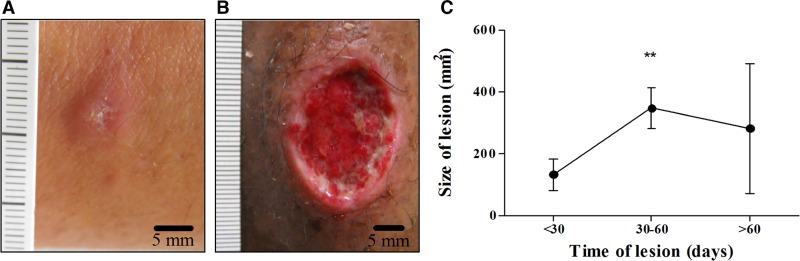
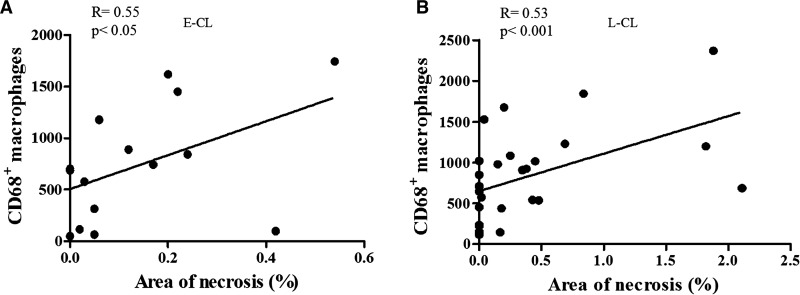
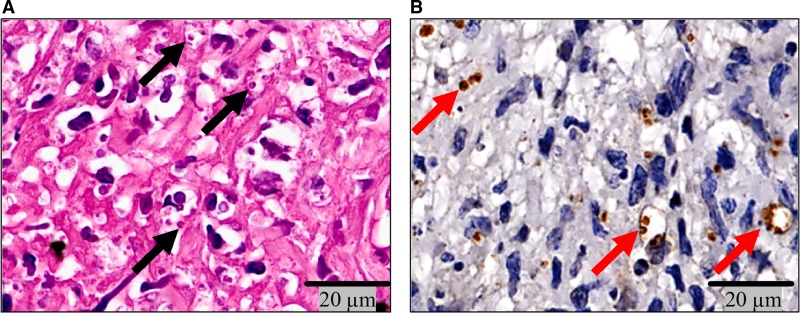
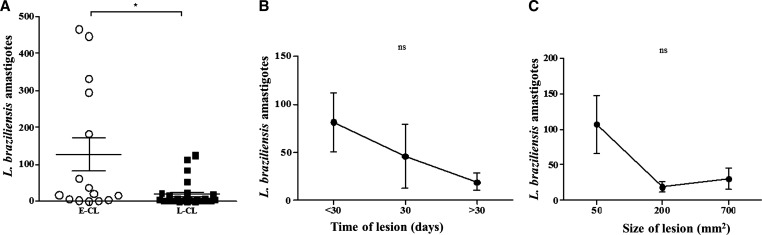
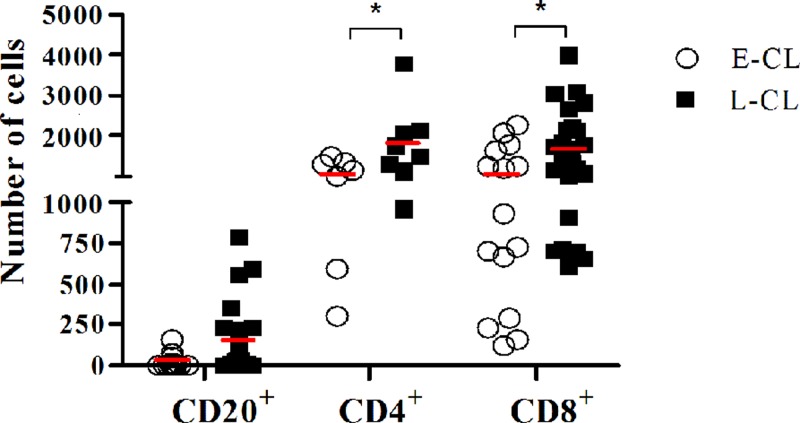
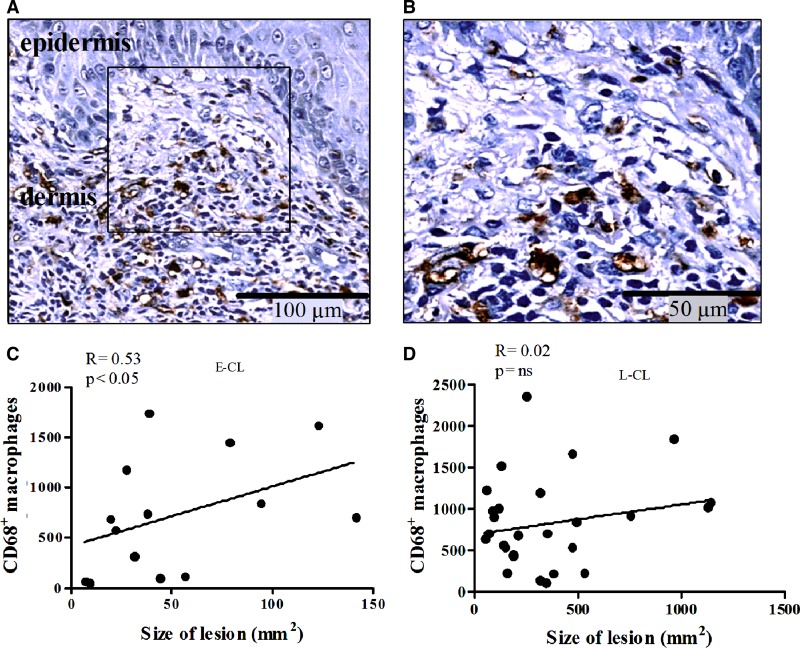
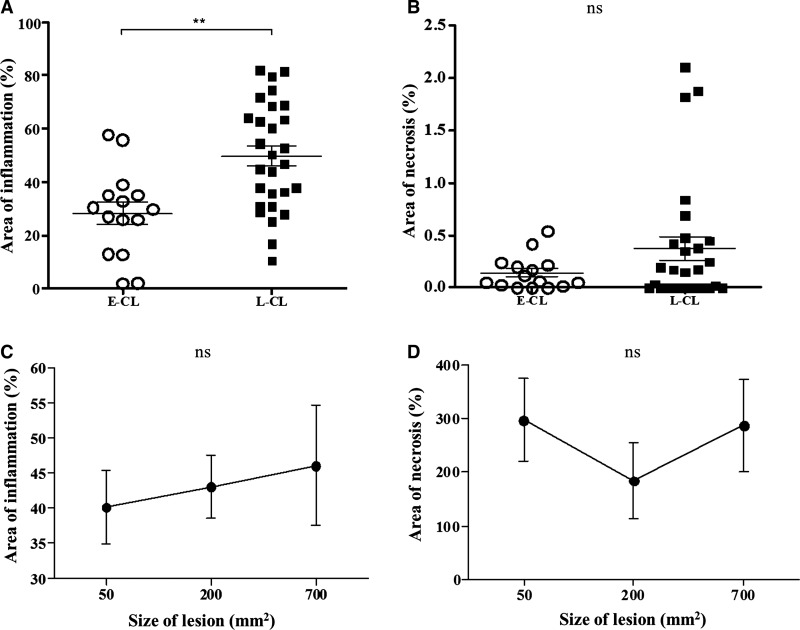
Cutaneous leishmaniasis (CL), characterized by an ulcerated lesion, is the most common clinical form of human leishmaniasis. Before the ulcer develops, patients infected with () present a small papule at the site of the sandfly bite, referred to as early cutaneous leishmaniasis (E-CL). Two to four weeks later the typical ulcer develops, which is considered here as late CL (L-CL). Although there is a great deal known about T-cell responses in patients with L-CL, there is little information about the in situ inflammatory response in E-CL. Histological sections of skin biopsies from 15 E-CL and 28 L-CL patients were stained by hematoxilin and eosin to measure the area infiltrated by cells, as well as tissue necrosis. amastigotes, CD4, CD8, CD20, and CD68 cells were identified and quantified by immunohistochemistry. The number of amastigotes in E-CL was higher than in L-CL, and the inflammation area was larger in classical ulcers than in E-CL. There was no relationship between the number of parasites and magnitude of the inflammation area, or with the lesion size. However, there was a direct correlation between the number of macrophages and the lesion size in E-CL, and between the number of macrophages and necrotic area throughout the course of the disease. These positive correlations suggest that macrophages are directly involved in the pathology of -induced lesions.
皮肤利什曼病(CL)以溃疡性病损为特征,是人类利什曼病最常见的临床形式。在溃疡形成之前,感染(此处原文括号内容缺失)的患者在白蛉叮咬部位会出现一个小丘疹,称为早期皮肤利什曼病(E-CL)。两到四周后,典型的溃疡形成,在此处被视为晚期CL(L-CL)。尽管关于L-CL患者的T细胞反应已有大量了解,但关于E-CL的原位炎症反应的信息却很少。对15例E-CL患者和28例L-CL患者的皮肤活检组织切片进行苏木精和伊红染色,以测量细胞浸润区域以及组织坏死情况。通过免疫组织化学鉴定并定量无鞭毛体、CD4、CD8、CD20和CD68细胞。E-CL中的无鞭毛体数量高于L-CL,经典溃疡中的炎症区域大于E-CL。寄生虫数量与炎症区域大小或病损大小之间没有关系。然而,在E-CL中,巨噬细胞数量与病损大小之间存在直接相关性,并且在疾病全过程中,巨噬细胞数量与坏死区域之间也存在直接相关性。这些正相关表明巨噬细胞直接参与了(此处原文缺失诱导因素)诱导的病损的病理过程。