Perrucci Elisabetta, Lancellotta Valentina, Benedetto Maika di, Palumbo Isabella, Matrone Fabio, Chiodi Marino, Lombi Riccardo, Marcantonini Marta, Mariucci Cristina, Aristei Cynthia
Radiation Oncology Section, Santa Maria della Misericordia Hospital.
Radiation Oncology Section, University of Perugia and Santa Maria della Misericordia Hospital.
J Contemp Brachytherapy. 2016 Dec;8(6):541-543. doi: 10.5114/jcb.2016.62958. Epub 2016 Oct 11.
Encrusted cystitis is a rare chronic inflammatory disease characterized by calcified plaques of the bladder, previously altered by varies conditions as urological procedures, caused by urea-splitting bacteria. Only one case has been reported on encrusted cystitis occurring after surgery and radiation therapy for a pelvic neoplasm. We report on encrusted cystitis occurred after definitive radiotherapy for bulky uterine cervix cancer, and examine the doses to the bladder wall and the procedure of radiation treatment performed as a possible cause of the onset of the disease.
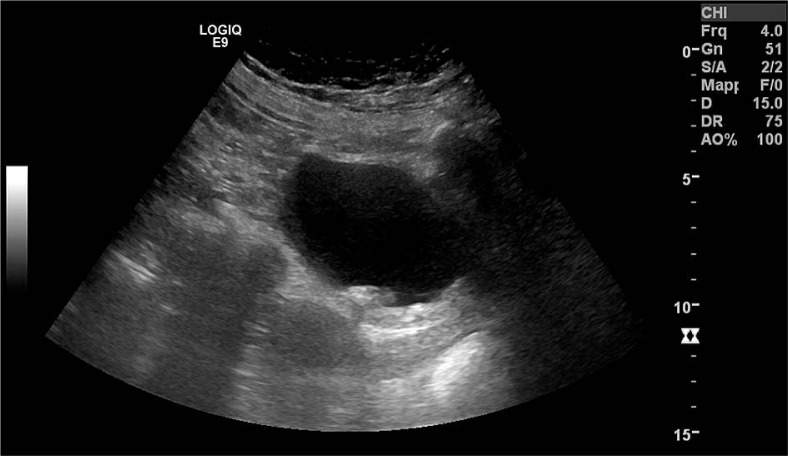
A 52-year-old female developed encrusted cystitis, caused by spp., after 14 months from definitive chemo-radiotherapy and 2/D brachytherapy treatment for FIGO stage IB2 uterine cervix cancer. For pelvic radiotherapy, the mean bladder dose was 48.47 Gy (range 31.20-51.91); maximal bladder point doses at each brachytherapy insertions were 7.62 Gy, 4.94 Gy and 6.27 Gy at first, second, and third fraction, respectively. Total biological effective dose (BED) at bladder point was 140.05 Gy. The patient was administered antibiotic therapy with linezolid and urine acidification with vitamin C; dietary norms were also suggested. After therapy, complete remission of symptoms and radiological findings were achieved, and the planned surgery for removing the calcified plaques was not completed. After 5 years from the cervical cancer diagnosis, the patient was disease-free without urinary symptoms.
The high doses administered to the bladder wall and the repeated catheterizations performed at each brachytherapy insertions may have favored the infection and promoted the occurrence of the encrusted cystitis.
结痂性膀胱炎是一种罕见的慢性炎症性疾病,其特征为膀胱出现钙化斑块,先前因各种情况如泌尿外科手术而改变,由尿素分解菌引起。仅有一例关于盆腔肿瘤手术后及放疗后发生结痂性膀胱炎的报道。我们报告了一例因巨大宫颈癌根治性放疗后发生的结痂性膀胱炎,并探讨膀胱壁所接受的剂量以及放疗程序作为该疾病发病可能原因的情况。
一名52岁女性在接受FIGO分期为IB2期宫颈癌的根治性放化疗及2/D近距离放疗14个月后,发生了由 菌属引起的结痂性膀胱炎。对于盆腔放疗,膀胱平均剂量为48.47 Gy(范围31.20 - 51.91);每次近距离放疗插入时膀胱最大点剂量在第一次、第二次和第三次分割时分别为7.62 Gy、4.94 Gy和6.27 Gy。膀胱点的总生物等效剂量(BED)为140.05 Gy。给予患者利奈唑胺抗生素治疗及维生素C酸化尿液;还建议了饮食规范。治疗后,症状和影像学表现完全缓解,且未完成计划的去除钙化斑块的手术。宫颈癌诊断5年后,患者无病且无泌尿系统症状。
膀胱壁所接受的高剂量以及每次近距离放疗插入时进行的反复导尿可能有利于感染并促进了结痂性膀胱炎的发生。