Duma M N, Heinrich C, Schönknecht C, Chizzali B, Mayinger M, Devecka M, Kampfer S, Combs S E
Department of Radiation Oncology, Klinikum rechts der Isar der Technischen Universität München, Ismaninger Str. 22, 81675, München, Germany.
Institute of Innovative Radiotherapy (iRT), Helmholtz Zentrum München, München, Germany.
Radiat Oncol. 2017 Jan 28;12(1):31. doi: 10.1186/s13014-016-0736-1.
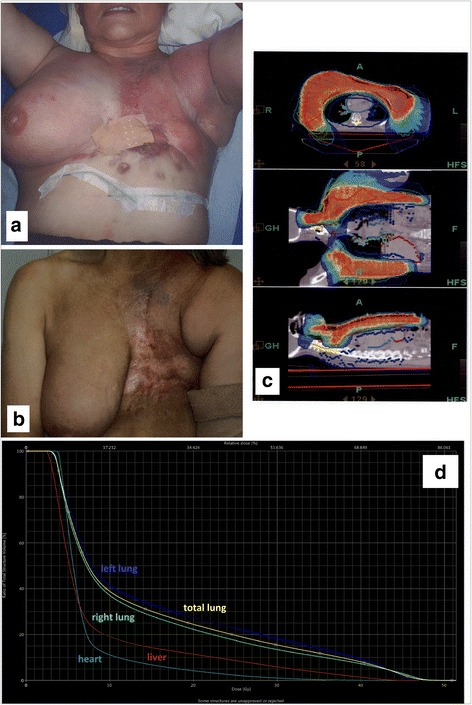
We report our experience of using helical tomotherapy (HT) to treat large and irregular shaped loco-regional advanced breast cancer target volumes embracing various organs at risk.
We retrospectively analyzed 26 patients treated for very large, irregular shaped breast cancers. Patients were treated either with the intent to achieve local control in a primary setting (n = 14) or in a reirradiation setting (n = 12). The recurrence group was heavily pretreated with systemic therapy. Tumors were characterized by wide infiltration of the skin, encompassing mostly a complete hemithorax. The primary group underwent irradiation of supraclavicular, infraclavicular, axillary and parasternal lymphonodal region. Radiotherapy was combined with chemotherapy (n = 11). We assessed the PTV volume and its craniocaudal extension, the dose to the organs at risk, acute toxicity and survival.
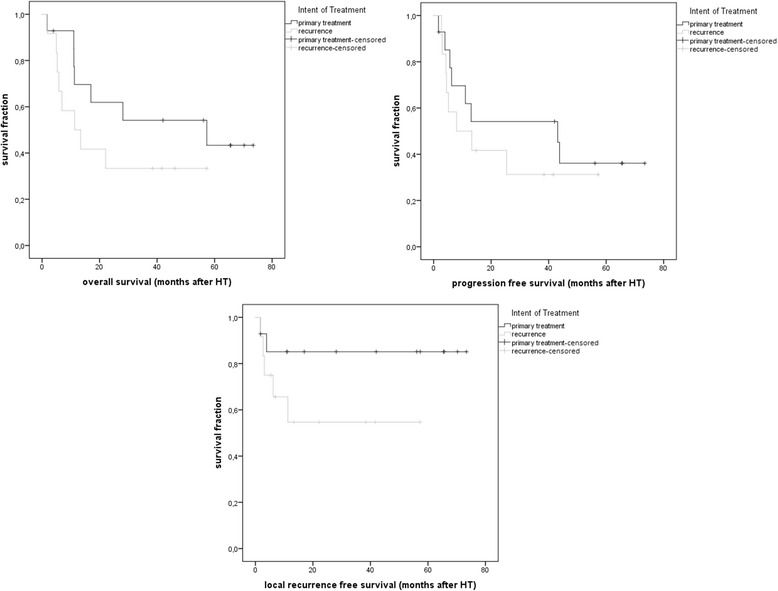
Median PTV was 2276 cm (1476-6837 cm) with a median cranio-caudal extension of 28 cm (15-52 cm). The median dose to PTV was 40 Gy (32-60Gy). HT could be carried out in all patients without interruption. The acute toxicities were mild to moderate. The median LRFS and OS after radiotherapy was 21 and 57 months for the primary group versus 10 and 11 months for the recurrence group. Median PFS was 18 months (primary group) and 7 months (recurrence group).
HT is feasible for advanced thorax embracing target volumes with acceptable acute toxicity. Both curative and palliative indications can be considered good indications based on treatment volume and anatomical constellation.
我们报告使用螺旋断层放射治疗(HT)治疗包含各种危及器官的大体积且形状不规则的局部区域晚期乳腺癌靶区的经验。
我们回顾性分析了26例接受治疗的体积非常大且形状不规则的乳腺癌患者。患者接受治疗的目的要么是在初始治疗时实现局部控制(n = 14),要么是在再程放疗时实现局部控制(n = 12)。复发组接受了大量的全身治疗。肿瘤的特征是皮肤广泛浸润,大多累及整个半侧胸部。初始组接受锁骨上、锁骨下、腋窝和胸骨旁淋巴结区域的照射。放疗联合化疗(n = 11)。我们评估了计划靶体积(PTV)及其头脚方向的延伸范围、危及器官的剂量、急性毒性和生存率。
PTV的中位数为2276 cm³(1476 - 6837 cm³),头脚方向的中位数延伸为28 cm(15 - 52 cm)。PTV的中位数剂量为40 Gy(32 - 60 Gy)。所有患者均可顺利进行HT治疗,无中断情况。急性毒性为轻至中度。放疗后,初始组的局部区域无复发生存期(LRFS)和总生存期(OS)的中位数分别为21个月和57个月,而复发组分别为10个月和11个月。无进展生存期(PFS)的中位数,初始组为18个月,复发组为7个月。
HT对于包含大体积靶区的晚期胸部肿瘤是可行的,急性毒性可接受。基于治疗体积和解剖结构,根治性和姑息性适应证均可视为良好适应证。