Morrell Stephen, Taylor Richard, Roder David, Robson Bridget, Gregory Marli, Craig Kirsty
School of Public Health and Community Medicine, University of NSW, Level 2, Samuels Building, Randwick, NSW, Australia.
Sansom Institute for Health Research, University of South Australia, Adelaide, SA, Australia.
Br J Cancer. 2017 Mar 14;116(6):828-839. doi: 10.1038/bjc.2017.6. Epub 2017 Feb 9.
This breast cancer mortality evaluation of service screening mammography in New Zealand, the first since commencement of screening in 1999, applies to the 1999-2011 diagnostic period. Individual-level linked information on mammography screening, breast cancer diagnosis and breast cancer mortality is used to analyse differences in breast cancer mortality according to participation in organised screening mammography, as provided by BreastScreen Aotearoa (BSA).
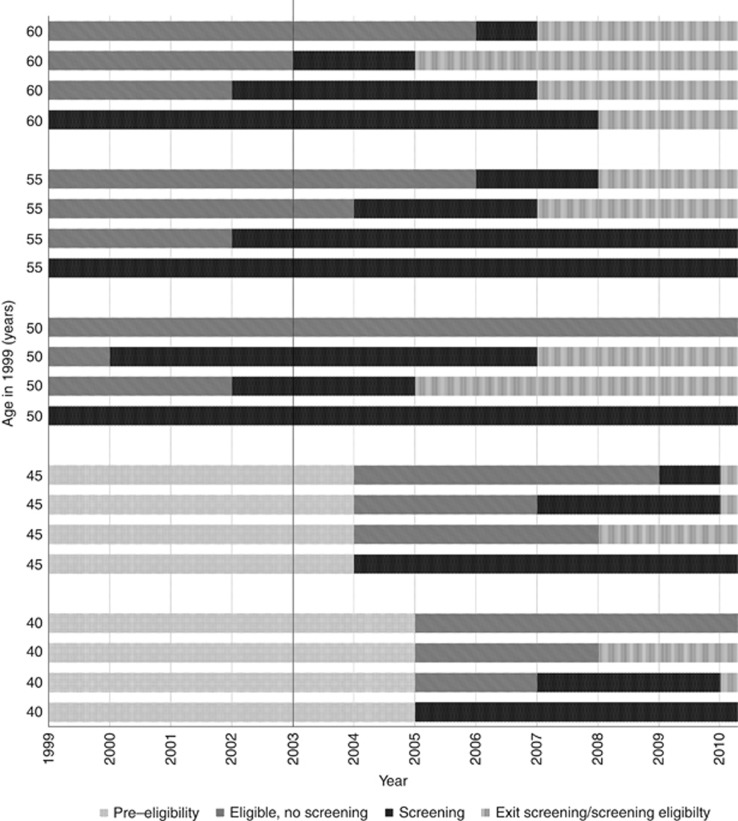
Women were followed from the time they became eligible for screening, from age 50 years (1999-2004) and 45 years (⩾2004). Breast cancer mortality from cancers diagnosed during the screening period from 1999 to 2011 (n=4384) is examined in relation to individual screening participation or non-participation during preceding person-years of follow-up from the time of screening eligibility. To account for changes from never- to ever-screened status, breast cancer mortality is calculated for each year in relation to prior accumulated time of participation and non-participation in screening. Breast cancer mortality is also examined in regularly screened women (screened ⩾3 times and mean screening interval ⩽30 months), and irregularly screened women compared with never-screened women. Statistical analyses are by negative binomial and Poisson regression with adjustment for age and ethnic group (Māori, Pacific women) in a repeated-measures analysis. Relative risks for breast cancer mortality compared with never-screened women, are adjusted also for screening selection bias, to indicate the extent of breast cancer mortality reduction in a population offered and not offered mammography screening. Prognostic indicators at diagnosis of breast cancer are also compared between different screening participation groups, including by grade of tumour, extent of disease (spread), multiple tumour status and maximum tumour size using χ statistics, t-tests and two-sample median tests.
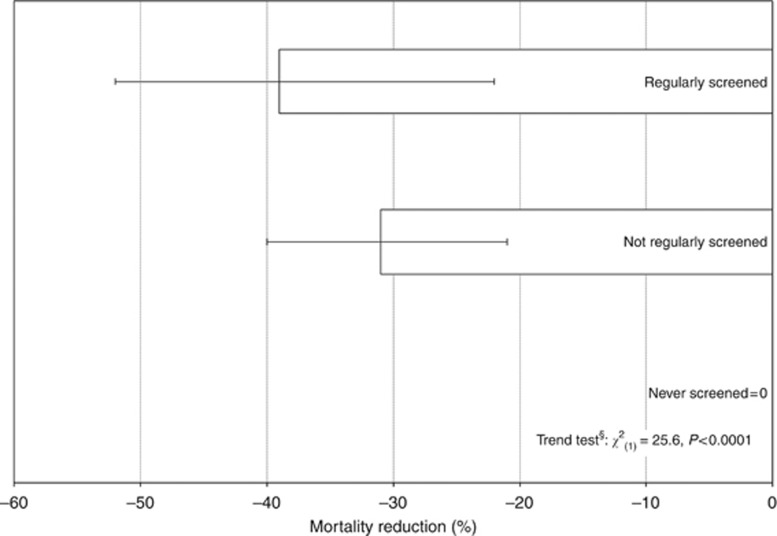
For 1999-2011, after adjusting for age and ethnicity, breast cancer mortality in ever-screened women is estimated to be 62% (95% CI: 51-70) lower than in never-screened women. After further adjustment for screening selection bias, the mortality reduction in NZ is estimated to be 29% (95% CI: 20-38) at an average screening coverage of 64% for 2001-2011, and 34% (95% CI: 25-43) for recent screening coverage (2012-13, 71%). For irregularly screened women, the mortality reduction is estimated to be 31% (95% CI: 21-40), and 39% (95% CI: 22-52) in regularly screened women compared with never-screened women, after adjusting for age, ethnicity and screening selection bias (using recent 2012-2013 screening coverage of 71%). Ever-screened women diagnosed with breast cancer have more favourable prognostic indicators than never-screened women, with a higher proportion of localised cancer (63 compared with 46%), a higher proportion with a well-differentiated tumour (30 compared with 18%), lower risk of multiple tumours (RR=0.48) and smaller median tumour size (15 mm compared with 20 mm)-all differences are statistically significant (P<0.0001).
This is the first total population cohort study of an established nation-wide screening mammography programme using individual-level information on screening participation and mortality outcomes from breast cancer. The findings are in accord with other mammography screening service evaluations and with randomised trials of mammography screening.
这是对新西兰乳腺钼靶筛查服务的乳腺癌死亡率评估,自1999年开始筛查以来首次进行,适用于1999 - 2011年诊断期。利用乳腺钼靶筛查、乳腺癌诊断和乳腺癌死亡率的个体层面关联信息,分析参与新西兰国家乳腺筛查机构(BSA)提供的有组织乳腺钼靶筛查与乳腺癌死亡率差异。
从女性符合筛查条件开始跟踪,1999 - 2004年为50岁,2004年及以后为45岁。研究1999年至2011年筛查期间确诊的癌症(n = 4384例)的乳腺癌死亡率与筛查资格确定后随访的前几年中个体筛查参与或未参与情况的关系。为了考虑从不筛查到曾筛查状态的变化,计算每年与之前累积的筛查参与和未参与时间相关的乳腺癌死亡率。还对定期筛查女性(筛查≥3次且平均筛查间隔≤30个月)和不定期筛查女性与未筛查女性的乳腺癌死亡率进行了研究。统计分析采用负二项式和泊松回归,并在重复测量分析中对年龄和种族(毛利人、太平洋岛民女性)进行调整。与未筛查女性相比,乳腺癌死亡率的相对风险也针对筛查选择偏倚进行了调整,以表明在提供和未提供乳腺钼靶筛查的人群中乳腺癌死亡率降低的程度。还使用χ²统计、t检验和两样本中位数检验比较了不同筛查参与组在乳腺癌诊断时的预后指标,包括肿瘤分级、疾病范围(扩散情况)、多肿瘤状态和最大肿瘤大小。
对于1999 - 2011年,在调整年龄和种族后,曾筛查女性的乳腺癌死亡率估计比未筛查女性低62%(95%CI:51 - 70)。在进一步调整筛查选择偏倚后,2001 - 2011年平均筛查覆盖率为64%时,新西兰的死亡率降低估计为29%(95%CI:20 - 38),近期筛查覆盖率(2012 - 13年,71%)时为34%(95%CI:25 - 43)。对于不定期筛查女性,在调整年龄、种族和筛查选择偏倚(使用2012 - 2013年近期筛查覆盖率71%)后,与未筛查女性相比,死亡率降低估计为31%(95%CI:21 - 40),定期筛查女性为39%(95%CI:22 - 52)。被诊断为乳腺癌的曾筛查女性比未筛查女性有更有利的预后指标,局部癌症比例更高(63%对比46%),高分化肿瘤比例更高(30%对比18%),多肿瘤风险更低(RR = 0.48),肿瘤中位数大小更小(15mm对比20mm)——所有差异均具有统计学意义(P < 0.0001)。
这是首次利用个体层面的筛查参与信息和乳腺癌死亡率结果,对已建立的全国性乳腺钼靶筛查项目进行的全人群队列研究。研究结果与其他乳腺钼靶筛查服务评估以及乳腺钼靶筛查随机试验结果一致。