Abram Michael E, Ram Renee R, Margot Nicolas A, Barnes Tiffany L, White Kirsten L, Callebaut Christian, Miller Michael D
Gilead Sciences, Foster City, California, United States of America.
PLoS One. 2017 Feb 17;12(2):e0172206. doi: 10.1371/journal.pone.0172206. eCollection 2017.
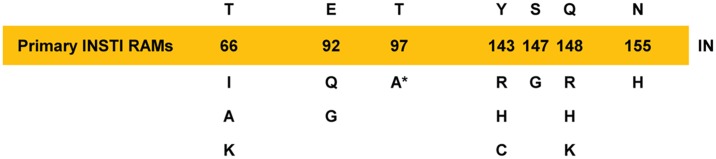
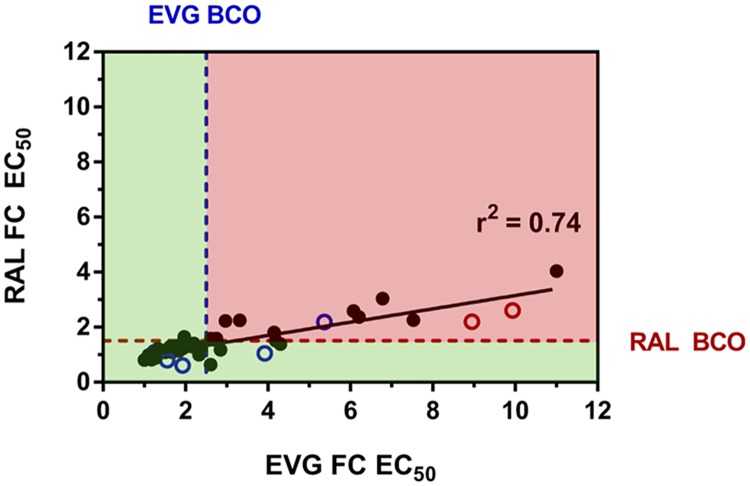
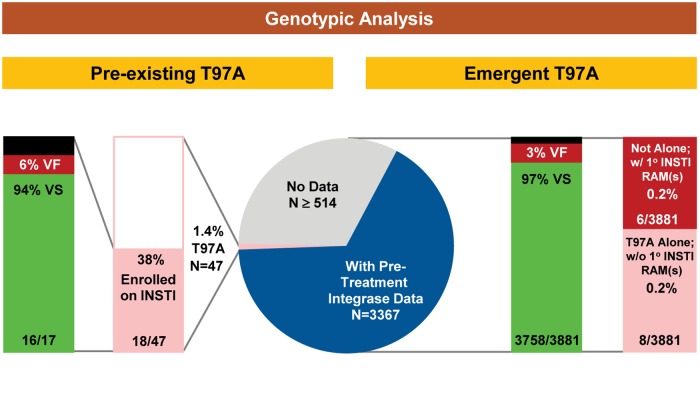
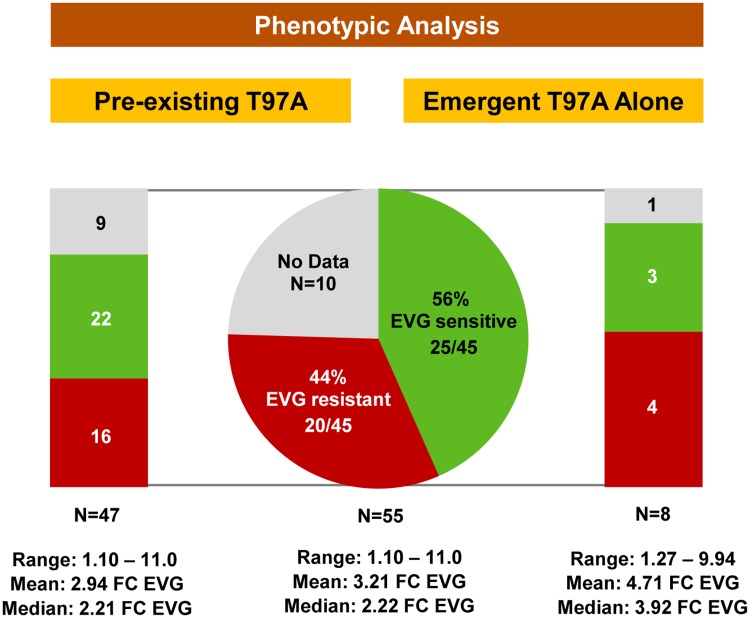
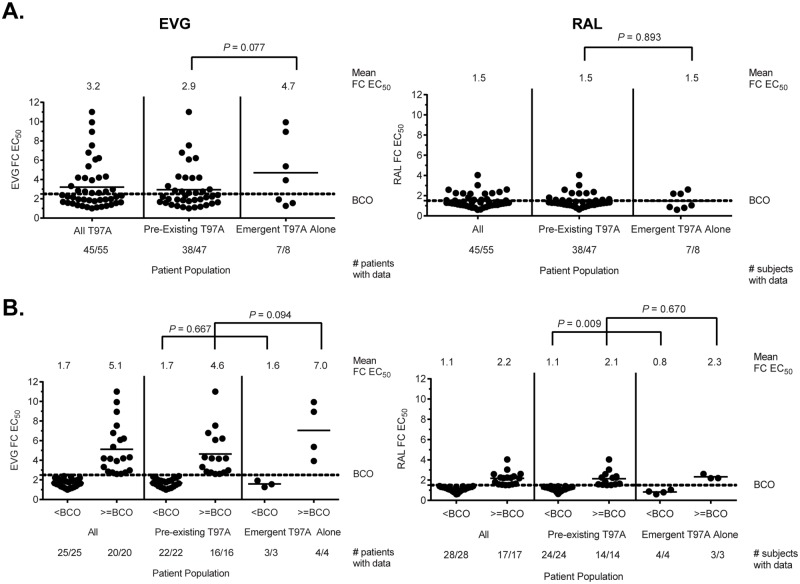
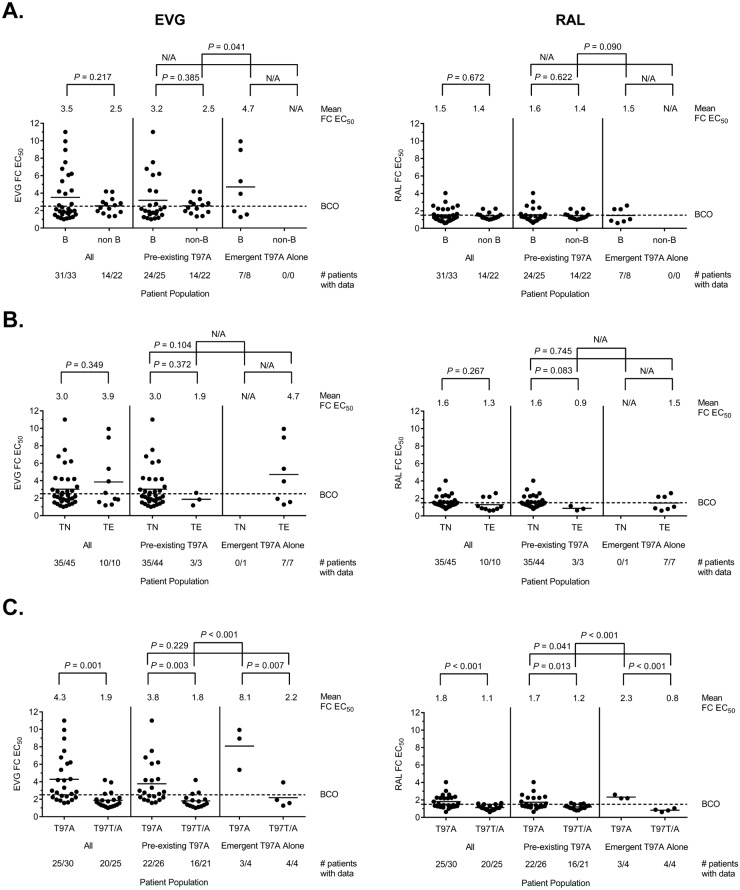
T97A is an HIV-1 integrase polymorphism associated with integrase strand transfer inhibitor (INSTI) resistance. Using pooled data from 16 clinical studies, we investigated the prevalence of T97A (pre-existing and emergent) and its impact on INSTI susceptibility and treatment response in INSTI-naive patients who enrolled on elvitegravir (EVG)- or raltegravir (RAL)-based regimens. Prior to INSTI-based therapy, primary INSTI resistance-associated mutations (RAMs) were absent and T97A pre-existed infrequently (1.4%; 47 of 3367 integrase sequences); most often among non-B (5.3%) than B (0.9%) HIV-1 subtypes. During INSTI-based therapy, few patients experienced virologic failure with emergent INSTI RAMs (3%; 122 of 3881 patients), among whom T97A emerged infrequently in the presence (n = 6) or absence (n = 8) of primary INSTI RAMs. A comparison between pre-existing and emergent T97A patient populations (i.e., in the absence of primary INSTI RAMs) showed no significant differences in EVG or RAL susceptibility in vitro. Furthermore, among all T97A-containing viruses tested, only 38-44% exhibited reduced susceptibility to EVG and/or RAL (all of low magnitude; <11-fold), while all maintained susceptibility to dolutegravir. Of the patients with pre-existing T97A, 17 had available clinical follow-up: 16 achieved virologic suppression and 1 maintained T97A and INSTI sensitivity without further resistance development. Overall, T97A is an infrequent integrase polymorphism that is enriched among non-B HIV-1 subtypes and can confer low-level reduced susceptibility to EVG and/or RAL. However, detection of T97A does not affect response to INSTI-based therapy with EVG or RAL. These results suggest a very low risk of initiating INSTI-based therapy in patients with pre-existing T97A.
T97A是一种与整合酶链转移抑制剂(INSTI)耐药相关的HIV-1整合酶多态性。利用来自16项临床研究的汇总数据,我们调查了T97A(基线存在和新发)的流行情况及其对初治患者接受基于埃替格韦(EVG)或拉替拉韦(RAL)方案治疗时INSTI敏感性和治疗反应的影响。在接受基于INSTI的治疗之前,主要的INSTI耐药相关突变(RAMs)不存在,T97A基线存在的情况很少见(1.4%;3367个整合酶序列中有47个);在非B型(5.3%)HIV-1亚型中比B型(0.9%)中更常见。在基于INSTI的治疗期间,很少有患者因新发INSTI RAMs而出现病毒学失败(3%;3881例患者中有122例),其中在存在(n = 6)或不存在(n = 8)主要INSTI RAMs的情况下,T97A新发的情况很少见。对基线存在和新发T97A患者群体(即不存在主要INSTI RAMs)进行比较,结果显示在体外对EVG或RAL的敏感性无显著差异。此外,在所有检测的含T97A病毒中,只有38 - 44%对EVG和/或RAL的敏感性降低(均为低水平;<11倍),而所有病毒对多替拉韦仍保持敏感性。在基线存在T97A的患者中,17例有可用的临床随访数据:16例实现了病毒学抑制,1例保持T97A和INSTI敏感性且未进一步出现耐药。总体而言,T97A是一种少见的整合酶多态性,在非B型HIV-1亚型中更为富集,可导致对EVG和/或RAL的低水平敏感性降低。然而,检测到T97A并不影响基于EVG或RAL的INSTI治疗反应。这些结果表明,对基线存在T97A的患者启动基于INSTI的治疗风险非常低。