Drewry Anne M, Ablordeppey Enyo A, Murray Ellen T, Stoll Carolyn R T, Izadi Sonya R, Dalton Catherine M, Hardi Angela C, Fowler Susan A, Fuller Brian M, Colditz Graham A
1Department of Anesthesiology, Washington University School of Medicine, St. Louis, MO. 2Departments of Emergency Medicine and Anesthesiology, Washington University School of Medicine, St. Louis, MO. 3University of Missouri-Columbia School of Medicine, Columbia, MO. 4Division of Public Health Sciences, Department of Surgery, Washington University School of Medicine, St. Louis, MO. 5Bernard Becker Medical Library, Washington University School of Medicine, St. Louis, MO.
Crit Care Med. 2017 May;45(5):806-813. doi: 10.1097/CCM.0000000000002285.
This meta-analysis aimed to examine the impact of antipyretic therapy on mortality in critically ill septic adults.
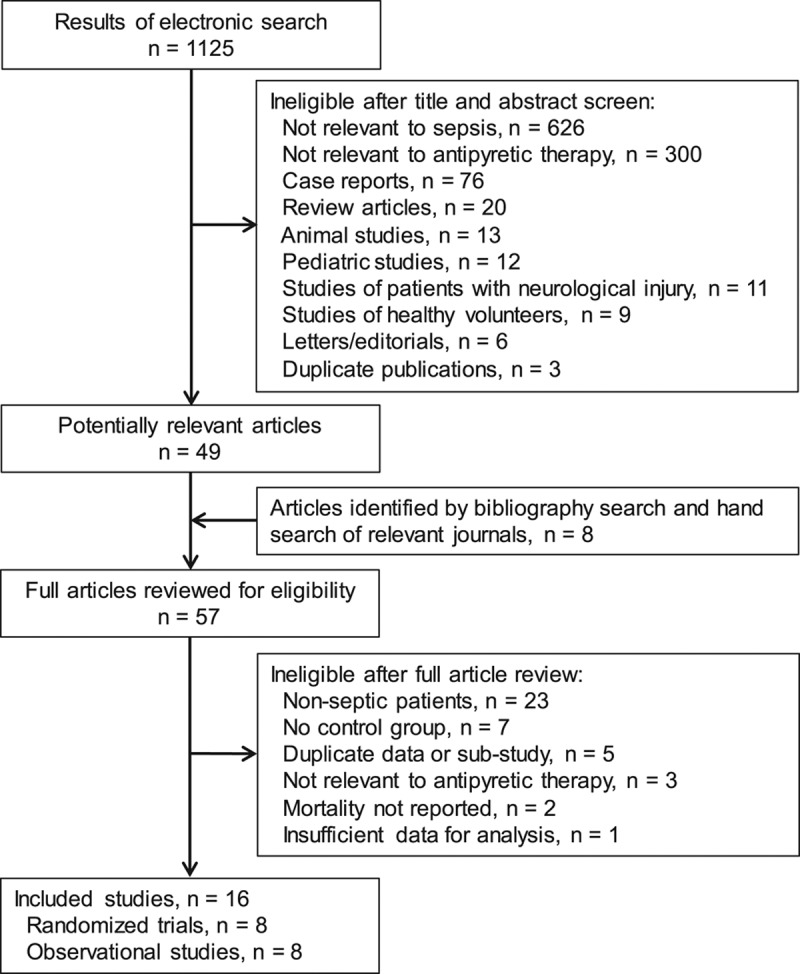
Literature searches were implemented in Ovid Medline, Embase, Scopus, Cumulative Index of Nursing and Allied Health Literature, Cochrane Central Register of Controlled Trials, NHS Economic Evaluation Database, and ClinicalTrials.gov through February 2016.
Inclusion criteria were observational or randomized studies of septic patients, evaluation of antipyretic treatment, mortality reported, and English-language version available. Studies were excluded if they enrolled pediatric patients, patients with neurologic injury, or healthy volunteers. Criteria were applied by two independent reviewers.
Two reviewers independently extracted data and evaluated methodologic quality. Outcomes included mortality, frequency of shock reversal, acquisition of nosocomial infections, and changes in body temperature, heart rate, and minute ventilation. Randomized and observational studies were analyzed separately.
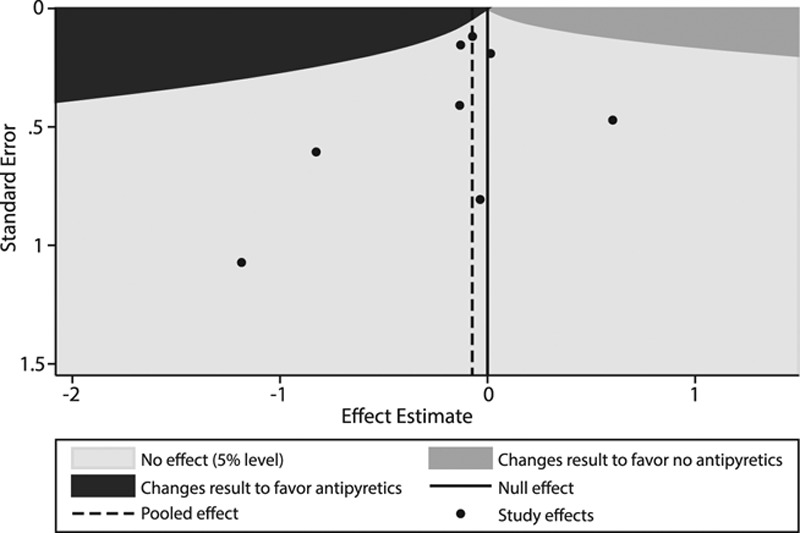
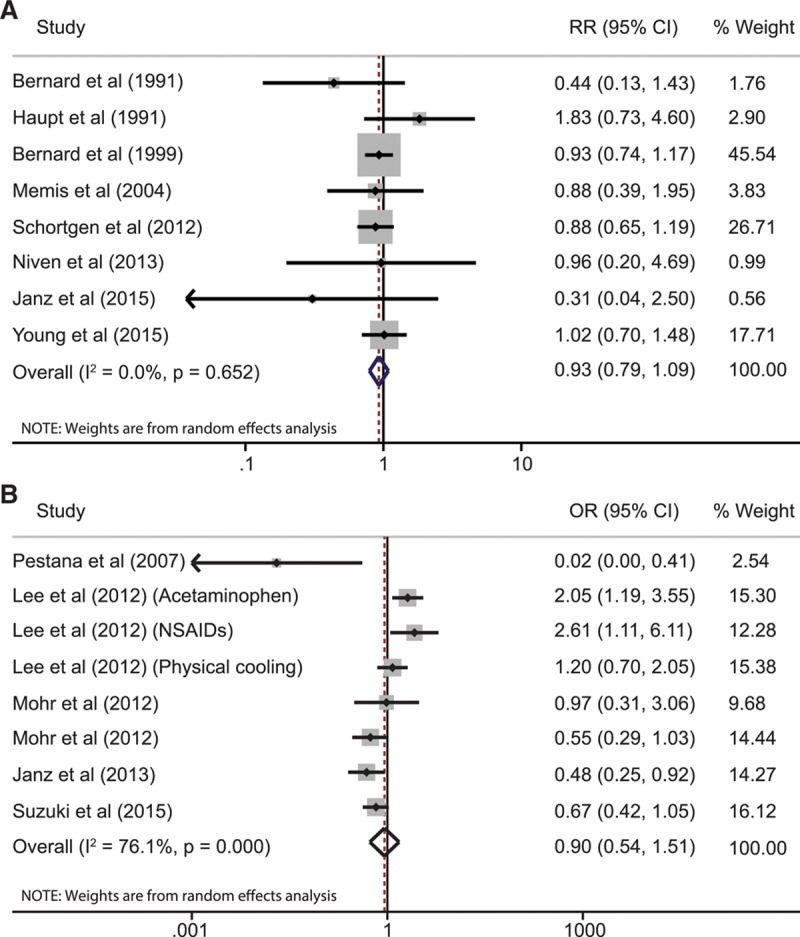
Eight randomized studies (1,507 patients) and eight observational studies (17,432 patients) were analyzed. Antipyretic therapy did not reduce 28-day/hospital mortality in the randomized studies (relative risk, 0.93; 95% CI, 0.77-1.13; I = 0.0%) or observational studies (odds ratio, 0.90; 95% CI, 0.54-1.51; I = 76.1%). Shock reversal (relative risk, 1.13; 95% CI, 0.68-1.90; I = 51.6%) and acquisition of nosocomial infections (relative risk, 1.13; 95% CI, 0.61-2.09; I = 61.0%) were also unchanged. Antipyretic therapy decreased body temperature (mean difference, -0.38°C; 95% CI, -0.63 to -0.13; I = 84.0%), but not heart rate or minute ventilation.
Antipyretic treatment does not significantly improve 28-day/hospital mortality in adult patients with sepsis.
本荟萃分析旨在研究退热治疗对重症脓毒症成年患者死亡率的影响。
截至2016年2月,通过检索Ovid Medline、Embase、Scopus、护理及相关健康文献累积索引、Cochrane对照试验中心注册库、英国国家卫生服务体系经济评估数据库及ClinicalTrials.gov获取文献。
纳入标准为脓毒症患者的观察性或随机研究、退热治疗评估、死亡率报告以及英文版本。若研究纳入儿科患者、神经损伤患者或健康志愿者则予以排除。由两名独立评审员应用该标准。
两名评审员独立提取数据并评估方法学质量。结局指标包括死亡率、休克逆转频率、医院获得性感染发生率以及体温、心率和分钟通气量的变化。随机研究和观察性研究分别进行分析。
分析了8项随机研究(1507例患者)和8项观察性研究(17432例患者)。在随机研究(相对危险度,0.93;95%可信区间,0.77 - 1.13;I² = 0.0%)或观察性研究(比值比,0.90;95%可信区间,0.54 - 1.51;I² = 76.1%)中,退热治疗均未降低28天/住院死亡率。休克逆转(相对危险度,1.13;95%可信区间,0.68 - 1.90;I² = 51.6%)和医院获得性感染发生率(相对危险度,1.13;95%可信区间,0.61 - 2.09;I² = 61.0%)也未改变。退热治疗可降低体温(平均差值,-0.38°C;95%可信区间,-0.63至-0.13;I² = 84.0%),但对心率或分钟通气量无影响。
退热治疗对成年脓毒症患者的28天/住院死亡率无显著改善。