Norton B L, Beitin A, Glenn M, DeLuca J, Litwin A H, Cunningham C O
Montefiore Medical Center, Albert Einstein College of Medicine, Division of General Internal Medicine, Bronx, NY, United States.
Montefiore Medical Center, Albert Einstein College of Medicine, Division of General Internal Medicine, Bronx, NY, United States.
J Subst Abuse Treat. 2017 Apr;75:38-42. doi: 10.1016/j.jsat.2017.01.015. Epub 2017 Jan 27.
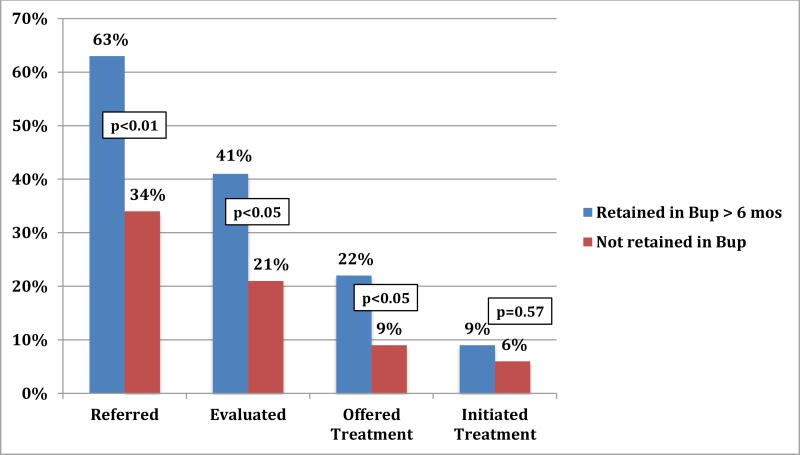
Persons who inject drugs, most of whom are opioid dependent, comprise the majority of the HCV infected in the United States. As the national opioid epidemic unfolds, increasing numbers of people are entering the medical system to access treatment for opioid use disorder, specifically with buprenorphine. Yet little is known about HCV care in patients accessing buprenorphine-based opioid treatment. We sought to determine the HCV prevalence, cascade of care, and the association between patient characteristics and completion of HCV cascade of care milestones for patients initiating buprenorphine treatment. We reviewed electronic health records of all patients who initiated buprenorphine treatment at a primary-care clinic in the Bronx, NY between January 2009 and January 2014. Of the 390 patients who initiated buprenorphine treatment, 123 were confirmed to have chronic HCV infection. The only patient characteristic associated with achieving HCV care milestones was retention in opioid treatment. Patients retained (vs. not retained) in buprenorphine treatment were more likely to be referred for HCV specialty care (63.1% vs. 34.0%, p<0.01), achieve an HCV-specific evaluation (40.8% vs. 21.3%, p<0.05), be offered HCV treatment (22.4% vs. 8.5%, p<0.05), and initiate HCV treatment (9.2% vs. 6.4%, p=0.6). Given the current opioid epidemic in the US and the growing number of people receiving buprenorphine treatment, there is an unprecedented opportunity to access and treat persons with HCV, reducing HCV transmission, morbidity and mortality. Retention in opioid treatment may improve linkage and retention in HCV care; innovative models of care that integrate opioid drug treatment with HCV treatment are essential.
注射毒品者(其中大多数对阿片类药物成瘾)占美国丙型肝炎病毒(HCV)感染者的大多数。随着全国性阿片类药物流行的发展,越来越多的人进入医疗系统以寻求阿片类药物使用障碍的治疗,特别是使用丁丙诺啡。然而,对于接受基于丁丙诺啡的阿片类药物治疗的患者的HCV护理情况知之甚少。我们试图确定开始丁丙诺啡治疗的患者的HCV患病率、护理流程以及患者特征与HCV护理流程各阶段完成情况之间的关联。我们回顾了2009年1月至2014年1月期间在纽约布朗克斯区一家初级保健诊所开始丁丙诺啡治疗的所有患者的电子健康记录。在开始丁丙诺啡治疗的390名患者中,有123人被确诊患有慢性HCV感染。与实现HCV护理各阶段目标相关的唯一患者特征是坚持接受阿片类药物治疗。坚持(与未坚持相比)接受丁丙诺啡治疗的患者更有可能被转诊至HCV专科护理(63.1%对34.0%,p<0.01)、接受HCV特异性评估(40.8%对21.3%,p<0.05)、获得HCV治疗(22.4%对8.5%,p<0.05)以及开始HCV治疗(9.2%对6.4%,p = 0.6)。鉴于美国当前的阿片类药物流行情况以及接受丁丙诺啡治疗的人数不断增加,存在前所未有的机会来诊治HCV患者,从而减少HCV传播、发病率和死亡率。坚持接受阿片类药物治疗可能会改善与HCV护理的联系及坚持程度;将阿片类药物治疗与HCV治疗相结合的创新护理模式至关重要。