4th Department of Internal Medicine, Medical School, National and Kapodistrian University of Athens, Athens, Greece.
Department of Clinical Chemistry and Laboratory Medicine, Jena University Hospital, Jena, Germany.
Crit Care. 2017 Mar 9;21(1):48. doi: 10.1186/s13054-017-1625-1.
Failure of circulating monocytes for adequate cytokine production is a trait of sepsis-induced immunosuppression; however, its duration and association with final outcome are poorly understood.
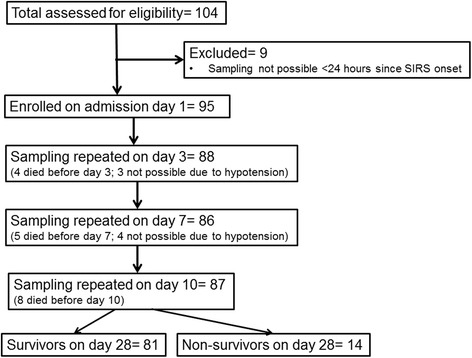
We conducted a substudy of a large randomised clinical trial. Peripheral blood mononuclear cells (PBMCs) were isolated within the first 24 h from the onset of systemic inflammatory response syndrome in 95 patients with microbiologically confirmed or clinically suspected gram-negative infections. Isolation was repeated on days 3, 7 and 10. PBMCs were stimulated for cytokine production. The study endpoints were the differences between survivors and non-survivors, the persistence of immunosuppression, and determination of admission clinical signs that can lead to early identification of the likelihood of immunosuppression.
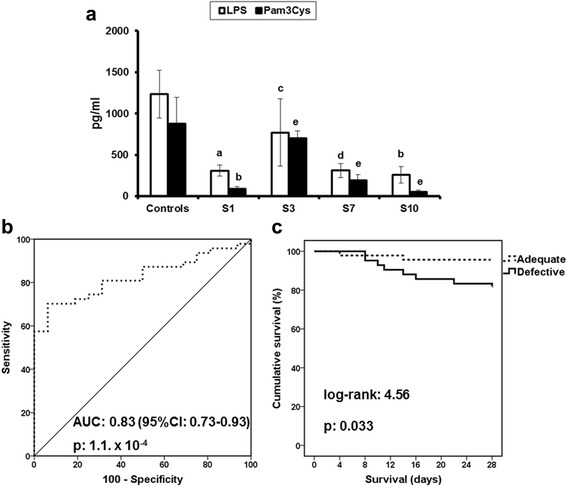
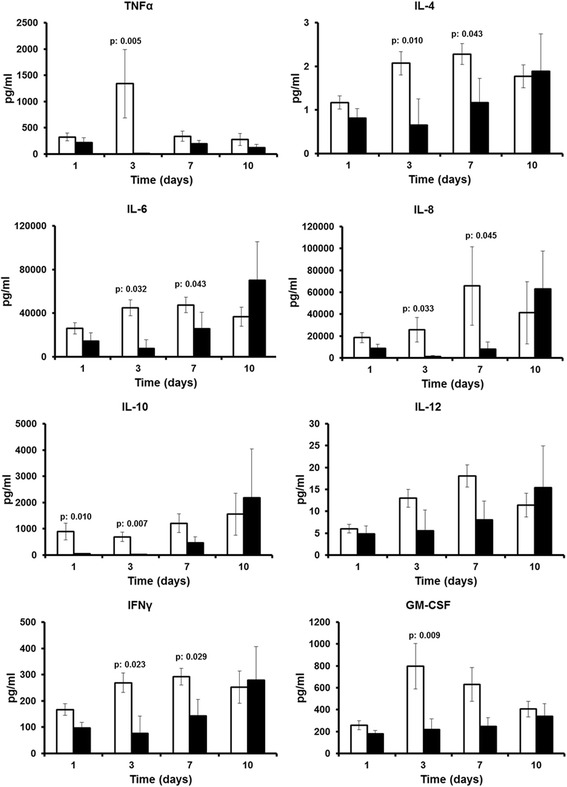
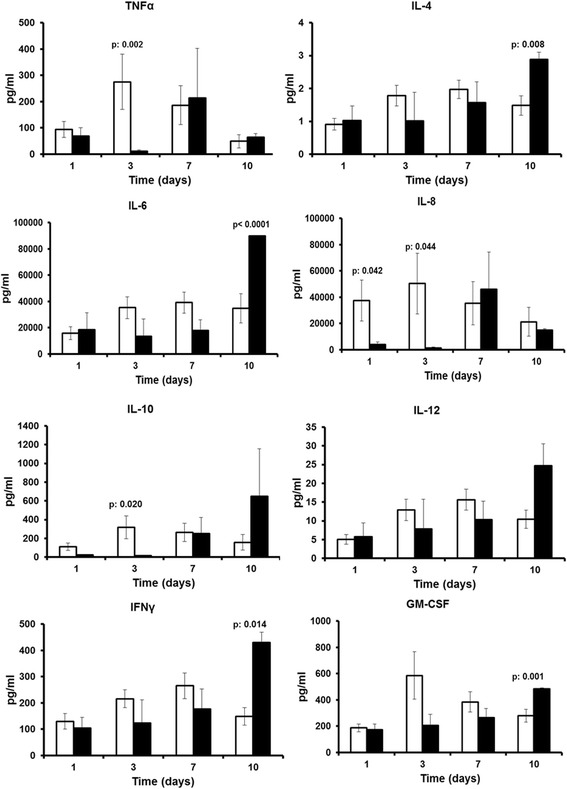
PBMCs of survivors produced significantly greater concentrations of tumour necrosis factor-α (TNF-α), interleukin (IL)-6, IL-8, IL-10, interferon-γ and granulocyte-macrophage colony-stimulating factor after day 3. Using ROC analysis, we found that TNF-α production less than 250 pg/ml after lipopolysaccharide stimulation on day 3 could discriminate patients from healthy control subjects; this was associated with a 5.18 OR of having an unfavourable outcome (p = 0.046). This trait persisted as long as day 10. Logistic regression analysis showed that cardiovascular failure on admission was the only independent predictor of defective TNF-α production on day 3.
Defective TNF-α production is a major trait of sepsis-induced immunosuppression. It is associated with significant risk for unfavourable outcome and persists until day 10. Cardiovascular failure on admission is predictive of defective TNF-α production during follow-up.
ClinicalTrials.gov identifier: NCT01223690 . Registered on 18 October 2010.
循环单核细胞无法充分产生细胞因子是脓毒症引起免疫抑制的特征;然而,其持续时间及其与最终结果的关联尚未得到很好的理解。
我们对一项大型随机临床试验进行了子研究。在 95 例微生物学证实或临床疑似革兰氏阴性感染患者全身炎症反应综合征发作的 24 小时内,从外周血单核细胞(PBMC)中分离出 PBMC。在第 3、7 和 10 天重复分离。刺激 PBMC 产生细胞因子。研究终点是幸存者和非幸存者之间的差异、免疫抑制的持续时间以及确定入院临床体征,以便早期识别免疫抑制的可能性。
幸存者的 PBMC 在第 3 天后产生的肿瘤坏死因子-α(TNF-α)、白细胞介素(IL)-6、IL-8、IL-10、干扰素-γ和粒细胞-巨噬细胞集落刺激因子的浓度明显更高。使用 ROC 分析,我们发现脂多糖刺激后第 3 天 TNF-α的产生低于 250pg/ml 可以区分患者与健康对照组;这与不良结局的 5.18 比值比(OR)相关(p=0.046)。这种特征一直持续到第 10 天。逻辑回归分析显示,入院时的心血管衰竭是第 3 天 TNF-α产生缺陷的唯一独立预测因子。
TNF-α产生缺陷是脓毒症引起免疫抑制的主要特征。它与不良结局的显著风险相关,并持续到第 10 天。入院时的心血管衰竭是预测随访期间 TNF-α产生缺陷的指标。
ClinicalTrials.gov 标识符:NCT01223690。于 2010 年 10 月 18 日注册。