Moss Travis J, Lake Douglas E, Calland J Forrest, Enfield Kyle B, Delos John B, Fairchild Karen D, Moorman J Randall
1Division of Cardiovascular Medicine, Department of Medicine, University of Virginia School of Medicine, Charlottesville, VA.2Department of Statistics, University of Virginia, Charlottesville, VA.3Division of Acute Care and Trauma Surgery, Department of Surgery, University of Virginia School of Medicine, Charlottesville, VA.4Division of Pulmonary and Critical Care, Department of Medicine, University of Virginia School of Medicine, Charlottesville, VA.5Department of Physics, College of William and Mary, Williamsburg, VA.6Division of Neonatology, Department of Pediatrics, University of Virginia School of Medicine, Charlottesville, VA.7Department of Biomedical Engineering, University of Virginia, Charlottesville, VA.8Department of Molecular Physiology, University of Virginia, Charlottesville, VA.
Crit Care Med. 2016 Sep;44(9):1639-48. doi: 10.1097/CCM.0000000000001738.
Patients in ICUs are susceptible to subacute potentially catastrophic illnesses such as respiratory failure, sepsis, and hemorrhage that present as severe derangements of vital signs. More subtle physiologic signatures may be present before clinical deterioration, when treatment might be more effective. We performed multivariate statistical analyses of bedside physiologic monitoring data to identify such early subclinical signatures of incipient life-threatening illness.
We report a study of model development and validation of a retrospective observational cohort using resampling (Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis type 1b internal validation) and a study of model validation using separate data (type 2b internal/external validation).
University of Virginia Health System (Charlottesville), a tertiary-care, academic medical center.
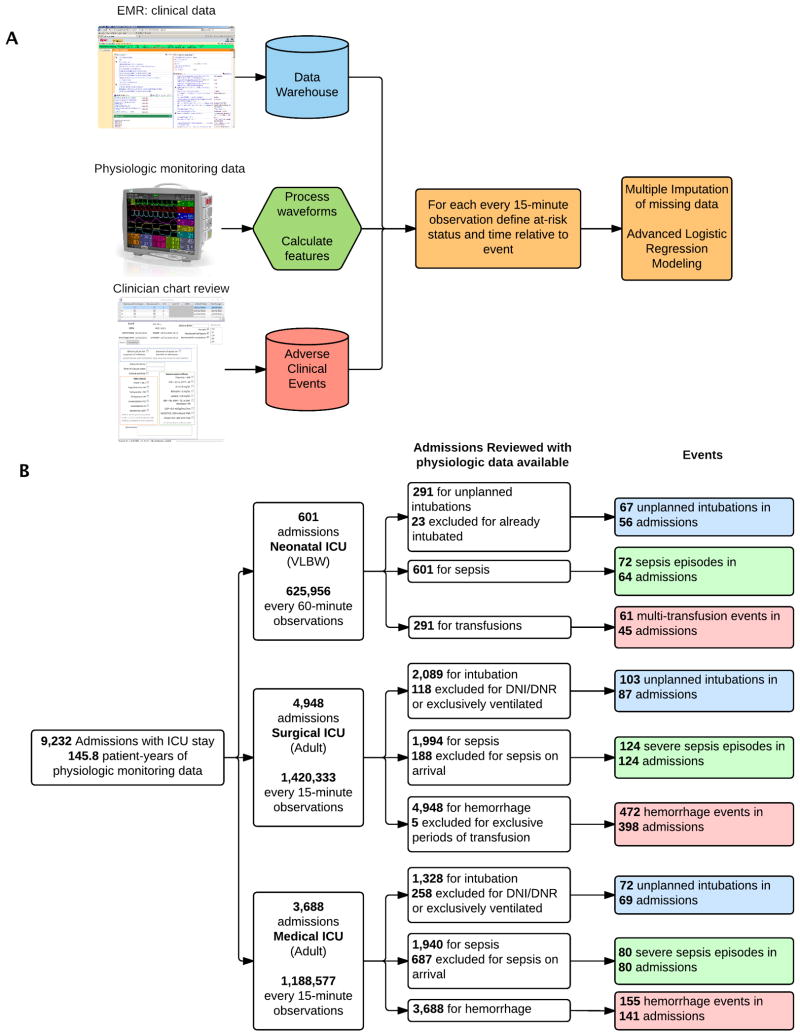
Critically ill patients consecutively admitted between January 2009 and June 2015 to either the neonatal, surgical/trauma/burn, or medical ICUs with available physiologic monitoring data.
None.
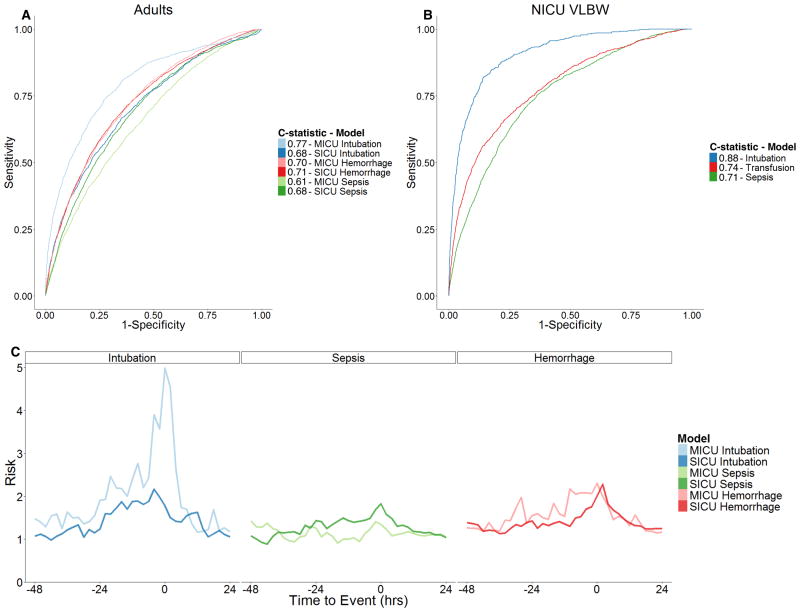
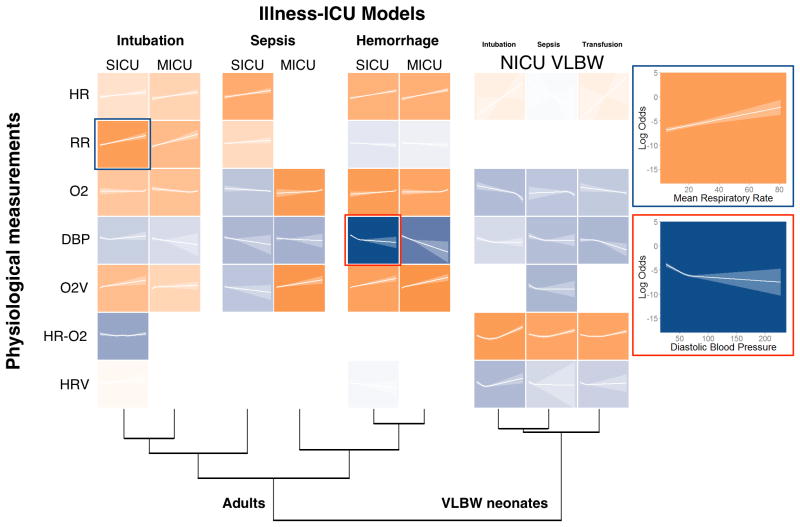
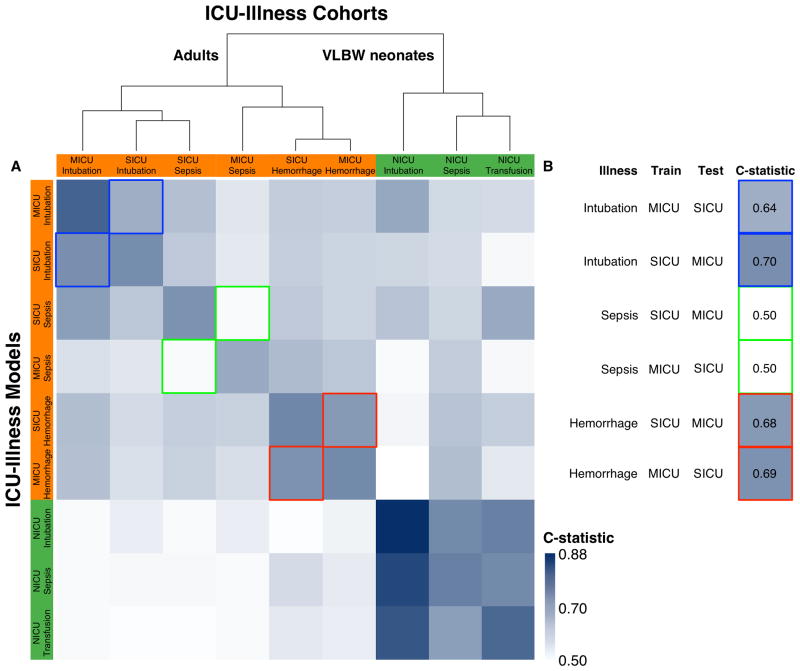
We analyzed 146 patient-years of vital sign and electrocardiography waveform time series from the bedside monitors of 9,232 ICU admissions. Calculations from 30-minute windows of the physiologic monitoring data were made every 15 minutes. Clinicians identified 1,206 episodes of respiratory failure leading to urgent unplanned intubation, sepsis, or hemorrhage leading to multi-unit transfusions from systematic individual chart reviews. Multivariate models to predict events up to 24 hours prior had internally validated C-statistics of 0.61-0.88. In adults, physiologic signatures of respiratory failure and hemorrhage were distinct from each other but externally consistent across ICUs. Sepsis, on the other hand, demonstrated less distinct and inconsistent signatures. Physiologic signatures of all neonatal illnesses were similar.
Subacute potentially catastrophic illnesses in three diverse ICU populations have physiologic signatures that are detectable in the hours preceding clinical detection and intervention. Detection of such signatures can draw attention to patients at highest risk, potentially enabling earlier intervention and better outcomes.
重症监护病房(ICU)的患者易患亚急性潜在灾难性疾病,如呼吸衰竭、脓毒症和出血,这些疾病表现为生命体征严重紊乱。在临床恶化之前可能会出现更细微的生理特征,此时进行治疗可能会更有效。我们对床边生理监测数据进行了多变量统计分析,以识别早期危及生命疾病的此类亚临床特征。
我们报告了一项使用重采样进行回顾性观察队列模型开发和验证的研究(个体预后或诊断多变量预测模型的透明报告类型1b内部验证)以及一项使用单独数据进行模型验证的研究(类型2b内部/外部验证)。
弗吉尼亚大学健康系统(夏洛茨维尔),一家三级医疗学术医学中心。
2009年1月至2015年6月期间连续入住新生儿、外科/创伤/烧伤或内科ICU且有可用生理监测数据的重症患者。
无。
我们分析了9232例ICU入院患者床边监测仪记录的146患者年生命体征和心电图波形时间序列。每15分钟对生理监测数据的30分钟窗口进行一次计算。临床医生通过系统的个体病历审查确定了1206例导致紧急非计划插管的呼吸衰竭发作、脓毒症或导致多单位输血的出血发作。预测未来24小时内事件的多变量模型内部验证的C统计量为0.61 - 0.88。在成人中,呼吸衰竭和出血的生理特征彼此不同,但在各ICU之间外部一致。另一方面,脓毒症表现出不太明显且不一致的特征。所有新生儿疾病的生理特征相似。
三种不同ICU人群中的亚急性潜在灾难性疾病具有在临床检测和干预前数小时可检测到的生理特征。检测到这些特征可以引起对高危患者的关注,有可能实现更早的干预并改善预后。