Mercado Chris Erwin G, Ekapirat Nattwut, Dondorp Arjen M, Maude Richard J
Mahidol Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand.
Department of Tropical Hygiene, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand.
Malar J. 2017 Mar 21;16(1):127. doi: 10.1186/s12936-017-1774-3.
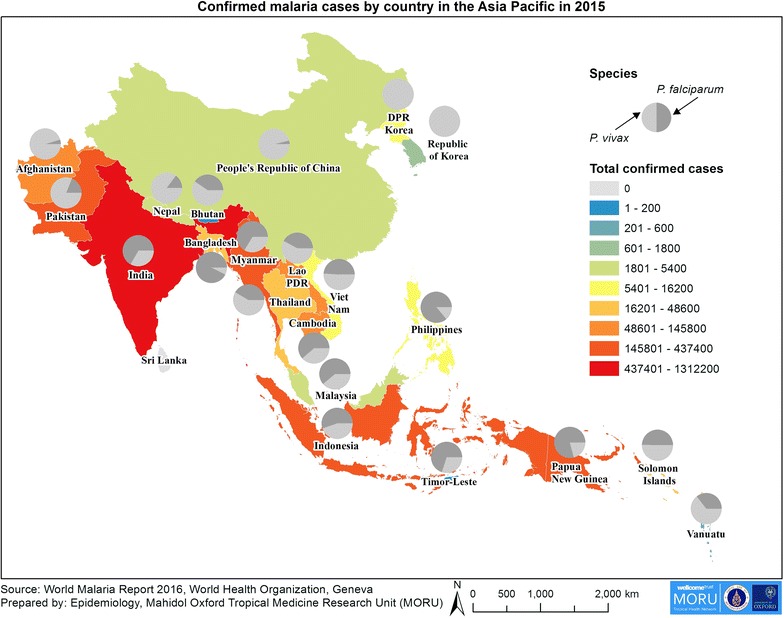
Heads of Government from Asia and the Pacific have committed to a malaria-free region by 2030. In 2015, the total number of confirmed cases reported to the World Health Organization by 22 Asia Pacific countries was 2,461,025. However, this was likely a gross underestimate due in part to incidence data not being available from the wide variety of known sources. There is a recognized need for an accurate picture of malaria over time and space to support the goal of elimination. A survey was conducted to gain a deeper understanding of the collection of malaria incidence data for surveillance by National Malaria Control Programmes in 22 countries identified by the Asia Pacific Leaders Malaria Alliance.
In 2015-2016, a short questionnaire on malaria surveillance was distributed to 22 country National Malaria Control Programmes (NMCP) in the Asia Pacific. It collected country-specific information about the extent of inclusion of the range of possible sources of malaria incidence data and the role of the private sector in malaria treatment. The findings were used to produce recommendations for the regional heads of government on improving malaria surveillance to inform regional efforts towards malaria elimination.
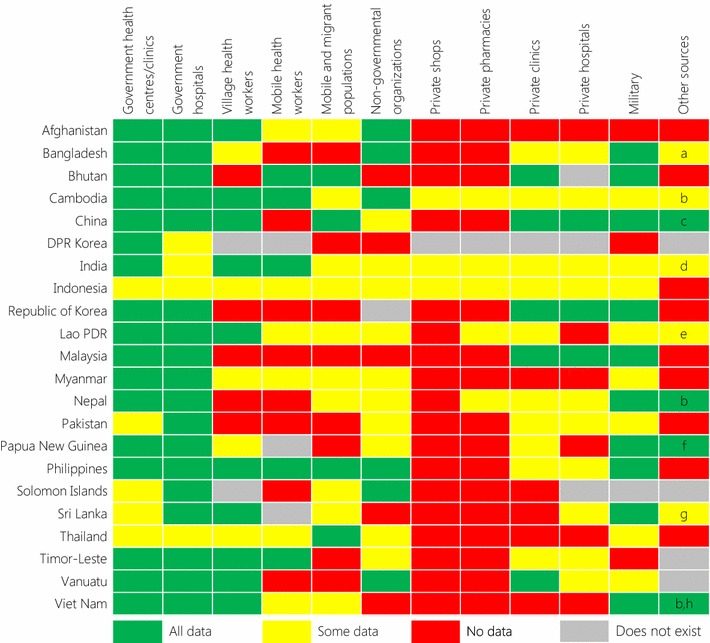
A survey response was received from all 22 target countries. Most of the malaria incidence data collected by NMCPs originated from government health facilities, while many did not collect comprehensive data from mobile and migrant populations, the private sector or the military. All data from village health workers were included by 10/20 countries and some by 5/20. Other sources of data included by some countries were plantations, police and other security forces, sentinel surveillance sites, research or academic institutions, private laboratories and other government ministries. Malaria was treated in private health facilities in 19/21 countries, while anti-malarials were available in private pharmacies in 16/21 and private shops in 6/21. Most countries use primarily paper-based reporting.
Most collected malaria incidence data in the Asia Pacific is from government health facilities while data from a wide variety of other known sources are often not included in national surveillance databases. In particular, there needs to be a concerted regional effort to support inclusion of data on mobile and migrant populations and the private sector. There should also be an emphasis on electronic reporting and data harmonization across organizations. This will provide a more accurate and up to date picture of the true burden and distribution of malaria and will be of great assistance in helping realize the goal of malaria elimination in the Asia Pacific by 2030.
亚太地区各国政府首脑已承诺到2030年实现无疟疾区域目标。2015年,22个亚太国家向世界卫生组织报告的确诊病例总数为2461025例。然而,这很可能是严重低估,部分原因是无法从各种已知来源获取发病率数据。人们认识到需要准确了解疟疾在时间和空间上的情况,以支持消除疟疾的目标。开展了一项调查,以更深入地了解亚太领导人疟疾联盟确定的22个国家的国家疟疾控制规划为监测目的收集疟疾发病率数据的情况。
2015 - 2016年,向亚太地区22个国家的国家疟疾控制规划发放了一份关于疟疾监测的简短问卷。问卷收集了各国关于疟疾发病率数据可能来源的纳入范围以及私营部门在疟疾治疗中的作用的具体信息。研究结果用于为地区政府首脑提出改进疟疾监测的建议,为该地区消除疟疾的努力提供参考。
收到了所有22个目标国家的调查回复。国家疟疾控制规划收集的大多数疟疾发病率数据源自政府卫生设施,而许多规划未从流动和移民人口、私营部门或军队收集全面数据。20个国家中有10个将乡村卫生工作者提供的所有数据纳入,5个国家部分纳入。一些国家纳入的其他数据来源包括种植园、警察和其他安全部队、哨点监测点、研究或学术机构、私人实验室以及其他政府部委。21个国家中有19个国家的私营卫生设施提供疟疾治疗,21个国家中有16个国家的私人药店有抗疟药出售,21个国家中有6个国家的私人商店有抗疟药出售。大多数国家主要采用纸质报告。
亚太地区收集的大多数疟疾发病率数据来自政府卫生设施,而来自各种其他已知来源的数据通常未纳入国家监测数据库。特别是,需要区域共同努力,支持纳入流动和移民人口以及私营部门的数据。还应强调电子报告和各组织间的数据协调统一。这将更准确、及时地反映疟疾的真实负担和分布情况,对助力实现亚太地区到2030年消除疟疾的目标大有帮助。