Borghs Simon, Thieffry Solène, Noack-Rink Matthias, Dedeken Peter, Hong Lai San, Byram Laura, Logan John, Chan Jane, Kiri Victor
UCB Pharma, Slough, UK.
UCB Pharma, Brussels, Belgium.
BMC Neurol. 2017 Mar 23;17(1):59. doi: 10.1186/s12883-017-0837-y.
Some antiepileptic drugs (AEDs) induce expression of hepatic enzymes. This can contribute to comorbidities via interference with metabolic pathways and concomitant drug metabolization, thereby increasing the likelihood of health care interventions. Using medical records, we compared the direct health care cost in patients initiating epilepsy therapy with enzyme-inducing AEDs (EIAEDs) vs non-enzyme-active AEDs (nEAAEDs) over up to 12 years.
Patients with untreated epilepsy were indexed in the UK Clinical Practice Research Datalink and Hospital Episode Statistics database when prescribed a new EIAED or nEAAED between January 2001 and December 2010. Propensity score matching reduced confounding factors between cohorts. Patients were followed until cohort treatment failure or data cut-off. The primary outcome was the median standardized monthly direct health care cost during follow-up in 2014 £GBP, calculated using published reference costs and compared using a Mann-Whitney U test.
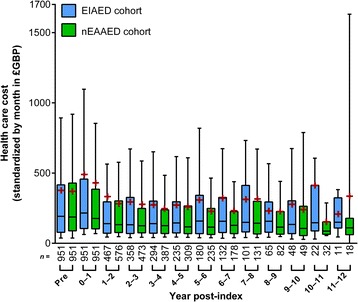
The unmatched EIAED cohort (n = 2752) was older (54 vs 46 years), more likely to be male, had more comorbidities, and higher health care resource use/cost during the 1-year pre-index period (median £3014 vs £2516) than the nEAAED cohort (n = 2,137). The most common index EIAED and nEAAED were carbamazepine (63.3%) and lamotrigine (58.0%), respectively. After matching, cohorts had similar features (n = 951 each). Over up to 12 years of follow-up, the median standardized monthly direct health care cost was £229 for the EIAED and £188 for the nEAAED cohorts (p = 0.0091). The median cost was higher for the EIAED cohort in every year of follow-up. In the two cohorts, 25.1% and 20.1% of total mean cost during follow-up was epilepsy-related, with approximately 4.6% and 3.0% for AED acquisition, respectively. The median time to cohort treatment failure was shorter in the matched EIAED cohort (468 vs 1194 days).
Patients in the UK who initiated epilepsy therapy with an EIAED appeared to be at higher risk of complications associated with enzyme induction. In long-term matched cohort analyses, the median total direct health care cost associated with EIAED therapy was higher than with nEAAEDs. Changing current treatment practices could potentially improve patient outcomes and reduce costs.
一些抗癫痫药物(AEDs)可诱导肝酶表达。这可能通过干扰代谢途径和伴随的药物代谢而导致合并症,从而增加医疗干预的可能性。我们利用医疗记录,比较了起始使用酶诱导型抗癫痫药物(EIAEDs)与非酶活性抗癫痫药物(nEAAEDs)进行癫痫治疗的患者长达12年的直接医疗费用。
2001年1月至2010年12月期间,在英国临床实践研究数据链和医院病历统计数据库中,将开始使用新的EIAED或nEAAED的未治疗癫痫患者作为研究对象。倾向评分匹配减少了队列之间的混杂因素。对患者进行随访,直至队列治疗失败或数据截止。主要结局是2014年英镑的随访期间标准化每月直接医疗费用中位数,使用已公布的参考成本计算,并采用Mann-Whitney U检验进行比较。
未匹配的EIAED队列(n = 2752)年龄更大(54岁对46岁),男性比例更高,合并症更多,在索引前1年的医疗资源使用/成本更高(中位数3014英镑对2516英镑),高于nEAAED队列(n = 2137)。最常用的索引EIAED和nEAAED分别是卡马西平(63.3%)和拉莫三嗪(58.0%)。匹配后,队列具有相似特征(每组n = 951)。在长达12年的随访中,EIAED队列标准化每月直接医疗费用中位数为229英镑,nEAAED队列中位数为188英镑(p = 0.0091)。在随访的每一年中,EIAED队列的费用中位数都更高。在两个队列中,随访期间总平均费用的25.1%和20.1%与癫痫相关,AED购置费用分别约为4.6%和3.0%。匹配后的EIAED队列中,队列治疗失败的中位时间更短(468天对1194天)。
在英国,起始使用EIAED进行癫痫治疗的患者似乎发生与酶诱导相关并发症的风险更高。在长期匹配队列分析中,与EIAED治疗相关的直接医疗费用中位数高于nEAAEDs。改变当前的治疗方法可能会改善患者预后并降低成本。