Mi Shu-Hua, Su Gong, Yang Hong-Xia, Zhou Yun, Tian Lei, Zhang Tao, Tao Hong
Center of Cardiology, Beijing An Zhen Hospital, Capital Medical University, No. 2 Anzhen Road, Chaoyang District, Beijing, China.
Department of Endocrinology, Beijing An Zhen Hospital, Capital Medical University, Beijing, China.
Diabetol Metab Syndr. 2017 Mar 21;9:20. doi: 10.1186/s13098-017-0217-1. eCollection 2017.
Admission hyperglycemia is associated with increased mortality and major adverse cardiac events (MACE) in patients with or without diabetes mellitus after acute myocardial infarction (AMI). However, effects of glycemic variability (GV) on outcomes of non-diabetes patients with AMI still remains unclear. The aim of this study is to compare the prognostic value of in-hospital GV with admission blood glucose (ABG) for 3-month MACE in non-diabetes patients with ST elevation myocardial infarction (STEMI) who underwent percutaneous coronary intervention (PCI).
We analyzed 256 non-diabetes patients with STEMI in study. The GV accessed by mean amplitude of glycemic excursions (MAGE) was calculated from blood glucose profiles of continuous glucose monitoring system (CGMS) during hospitalization. ABG was measured on admission. Main endpoints were 3-month MACE; secondary endpoints were GRACE scores and enzymatic infarct size. Predictive effects of MAGE and ABG on the MACE in patients were analyzed.
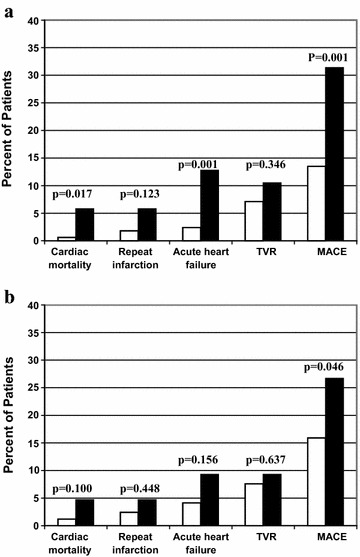
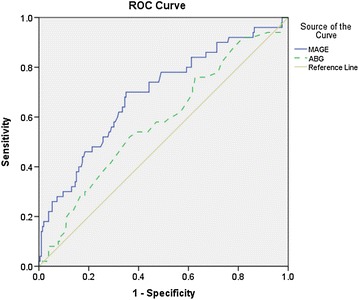
In all participants, MAGE level was associated with ABG level (r = 0.242, p < 0.001). Both elevated MAGE levels (p = 0.001) and elevated ABG (p = 0.046) were associated with incidences of short-term MACE. Patients with a higher MAGE level had a significantly higher cardiac mortality (5.8 vs. 0.6%, p = 0.017) and incidence of acute heart failure (12.8 vs. 2.4%, p = 0.001) during 3 months follow-up. In multivariable analysis, high MAGE level (HR 2.165, p = 0.023) was significantly associated with incidence of short-term MACE, but ABG (HR 1.632, p = 0.184) was not. The area under the receiver-operating characteristic curve for MAGE (0.690, p < 0.001) was superior to that for ABG (0.581, p = 0.076).
To compare with ABG, in-hospital GV may be a more important predictor of short-term MACE and mortality in non-diabetes patients with STEMI treated with PCI.
急性心肌梗死(AMI)后,无论有无糖尿病,入院时高血糖均与死亡率增加及主要不良心脏事件(MACE)相关。然而,血糖变异性(GV)对非糖尿病AMI患者预后的影响仍不明确。本研究旨在比较住院期间GV与入院血糖(ABG)对接受经皮冠状动脉介入治疗(PCI)的非糖尿病ST段抬高型心肌梗死(STEMI)患者3个月MACE的预后价值。
我们分析了研究中的256例非糖尿病STEMI患者。住院期间通过连续血糖监测系统(CGMS)的血糖谱计算平均血糖波动幅度(MAGE)来评估GV。入院时测量ABG。主要终点为3个月MACE;次要终点为GRACE评分和酶学梗死面积。分析MAGE和ABG对患者MACE的预测作用。
在所有参与者中,MAGE水平与ABG水平相关(r = 0.242,p < 0.001)。MAGE水平升高(p = 0.001)和ABG升高(p = 0.046)均与短期MACE发生率相关。MAGE水平较高的患者在3个月随访期间心脏死亡率显著更高(5.8%对0.6%,p = 0.017),急性心力衰竭发生率也显著更高(12.8%对2.4%,p = 0.001)。在多变量分析中,高MAGE水平(HR 2.165,p = 0.023)与短期MACE发生率显著相关,但ABG(HR 1.632,p = 0.184)则不然。MAGE的受试者工作特征曲线下面积(0.690,p < 0.001)优于ABG(0.581,p = 0.076)。
与ABG相比,住院期间GV可能是接受PCI治疗的非糖尿病STEMI患者短期MACE和死亡率的更重要预测指标。