Müller-Hagedorn Silvia, Buchenau Wolfgang, Arand Jörg, Bacher Margit, Poets Christian F
Interdisciplinary Centre for Craniofacial Malformations, Tuebingen University Hospital, Calwerstrasse 7, 72076, Tuebingen, Germany.
Department of Neonatology, Tuebingen University Hospital, Calwerstrasse 7, 72076, Tuebingen, Germany.
Head Face Med. 2017 Mar 30;13(1):4. doi: 10.1186/s13005-017-0137-1.
Infants with Robin sequence (RS) suffer from upper airway obstruction (UAO) and feeding problems. We developed an oral appliance with a velar extension in combination with functional treatment and appropriate feeding techniques, which was proven effective in isolated RS. As the above problems are particularly challenging in syndromic RS, we set out to evaluate our treatment concept also in these patients.
We searched our electronic departmental database to identify all children admitted to our department between 01/01/2003 and 31/12/2009 because of syndromic RS. UAO was quantified by cardiorespiratory sleep studies performed before and during treatment with a modified palatal plate. This appliance consists of a palatal part, covering the hard palate as well as the alveolar ridges and the potential cleft, and a velar extension shifting the tongue in a more anterior position, thereby opening the pharyngeal airway. It is adjusted by fiberoptic nasopharyngoscopy and controlled by cardiorespiratory sleep studies. Obstructive sleep apnea was defined as a mixed obstructive sleep apnea index (MOAI) >3/h. Feeding modalities before and after treatment and weight gain, determined as standard deviation score, were also evaluated.
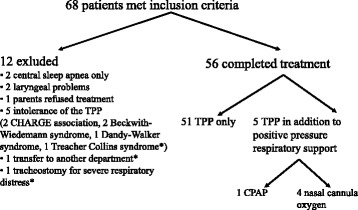
Of 68 children meeting inclusion criteria, 56 completed treatment (46 of these being infants). Underlying diagnoses included craniofacial dysostosis (N = 13) and synostosis syndromes (N = 5), unspecified dysmorphic syndromes (N = 23) and miscellaneous rare conditions (N = 27). Median MOAI decreased from 8.5 (range 0.3-76.0) at admission to 1.1 (0.0-5.2) at discharge (p < 0.001). 51 children received only a TPP and 5 additionally continuous positive airway pressure (CPAP) or high-flow nasal cannula during sleep for mild residual OSA. Three children ultimately required tracheostomy. The number of exclusively gavage fed infants was reduced from 23 to 7. Conversely, the number of children fed exclusively by mouth increased from 18 to 30. Median SDS for weight decreased from -1.6 (-3.5-1.7) to -1.3 (-4.1-2.5). Twelve children had their treatment prematurely discontinued, e.g. due to laryngeal collapse/laryngomalacia. No patient died during treatment.
Treatment of UAO and feeding problems in these children with syndromic RS by a modified palatal plate with a velar extension was shown to be effective and safe. If confirmed in prospective studies, it may help to avoid more invasive interventions.
患有罗宾序列征(RS)的婴儿存在上呼吸道梗阻(UAO)和喂养问题。我们研发了一种带有软腭延伸部分的口腔矫治器,并结合功能治疗和适当的喂养技巧,已证实该方法对单纯性RS有效。由于上述问题在综合征性RS中尤其具有挑战性,我们着手评估在这些患者中应用我们的治疗理念的效果。
我们检索了科室的电子数据库,以确定2003年1月1日至2009年12月31日期间因综合征性RS入住我科的所有儿童。通过在使用改良腭板治疗前和治疗期间进行的心肺睡眠研究对UAO进行量化。该矫治器由覆盖硬腭、牙槽嵴和潜在腭裂的腭部以及将舌头向前移位从而打开咽气道的软腭延伸部分组成。通过纤维鼻咽喉镜进行调整,并由心肺睡眠研究进行监测。阻塞性睡眠呼吸暂停被定义为混合性阻塞性睡眠呼吸暂停指数(MOAI)>3次/小时。还评估了治疗前后的喂养方式以及以标准差评分确定的体重增加情况。
在68名符合纳入标准的儿童中,56名完成了治疗(其中46名是婴儿)。潜在诊断包括颅面骨发育不全(N = 13)和颅骨缝早闭综合征(N = 5)未明确的畸形综合征(N = 23)以及其他罕见病症(N = 27)。MOAI中位数从入院时的8.5(范围0.3 - 76.0)降至出院时的1.1(0.0 - 5.2)(p < 0.001)。51名儿童仅接受了改良腭板治疗,5名儿童因轻度残余阻塞性睡眠呼吸暂停在睡眠期间额外接受了持续气道正压通气(CPAP)或高流量鼻导管通气。3名儿童最终需要进行气管切开术。完全通过管饲喂养的婴儿数量从23名减少至7名。相反,完全经口喂养的儿童数量从18名增加至30名。体重的中位数标准差评分从 -1.6(-3.5 - 1.7)降至 -1.3(-4.1 - 2.5)。12名儿童过早中断治疗,例如由于喉塌陷/喉软化。治疗期间无患者死亡。
采用带有软腭延伸部分的改良腭板治疗这些患有综合征性RS的儿童的UAO和喂养问题被证明是有效且安全的。如果在前瞻性研究中得到证实,可能有助于避免更具侵入性的干预措施。