Department of Oral and Maxillofacial Surgery, 14903Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, Germany.
Department of Phoniatrics & Pedaudiology, 14903Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, Germany.
Cleft Palate Craniofac J. 2021 Aug;58(8):1063-1069. doi: 10.1177/1055665620972288. Epub 2020 Nov 11.
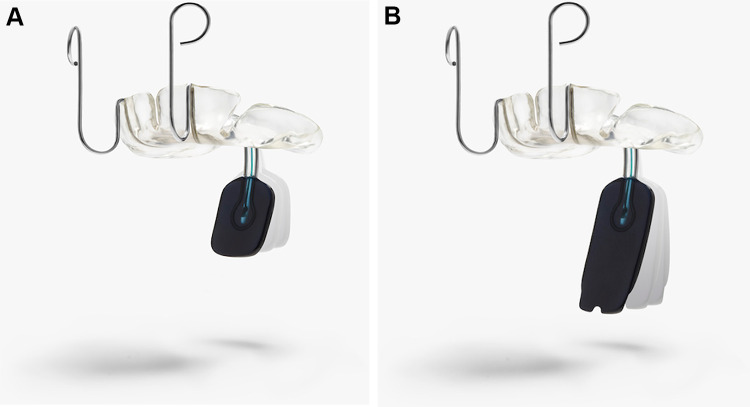
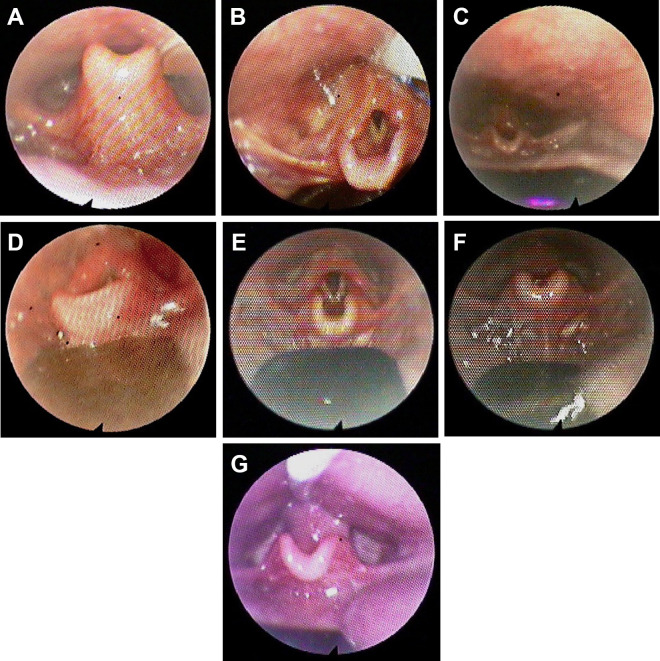
Despite its efficiency and benefits in treating patients with Robin sequence (RS), the pre-epiglottic baton plate (PEBP) is not widely used. However, its acceptance might improve with specific defined parameters for indication and proper design of the velar extension. We present our 13-year, single-center experience in treating infants with RS using PEBP, focusing on the description and insertion of an endoscopically guided PEBP design along with its complications and limitations.
We recommend PEBP as primary treatment for RS, suggesting a new approach of design adjustment based on endoscopic findings of multilevel upper airway obstruction.
Department of cleft lip and palate.
Infants with isolated or syndromic RS, period 2010 to 2019.
Pre-epiglottic baton plate treatment, intravelar veloplasty, and hard palate closure after initial PEBP treatment.
We treated 132 infants (isolated RS, 111; syndromic RS, 21) with PEBP. All infants with isolated RS were discharged within an average of 8 days of PEBP therapy. For them, no tracheotomy or tongue-lip adhesion procedures were needed. Only 4 of the 20 infants discharged with a nasogastric tube needed it for >2 weeks. Intravelar veloplasty and palate closure were performed after 3 and 6 months of initiating PEBP treatment, respectively.
Application of an orthodontic device in RS therapy has not been accepted worldwide. We hope that our learning curve and recommendations about PEBP will help the implementation of this highly effective and nonsurgical treatment option.
尽管预会厌棒板(PEBP)在治疗 Robin 序列(RS)患者方面具有高效性和益处,但并未得到广泛应用。然而,随着其适应证的特定明确参数和软腭延伸的合理设计,其接受度可能会提高。我们介绍了我们在单中心治疗 RS 婴儿的 13 年经验,重点介绍了经内镜引导的 PEBP 设计的描述和插入,以及其并发症和局限性。
我们建议将 PEBP 作为 RS 的主要治疗方法,建议根据多水平上气道阻塞的内镜检查结果,采用新的设计调整方法。
腭裂科室。
患有孤立性或综合征性 RS 的婴儿,时间为 2010 年至 2019 年。
PEBP 治疗、内软腭裂成形术和初始 PEBP 治疗后的硬腭裂闭合术。
我们用 PEBP 治疗了 132 名婴儿(孤立性 RS,111 例;综合征性 RS,21 例)。所有孤立性 RS 婴儿平均在 8 天内接受 PEBP 治疗后出院。他们中没有需要气管切开术或舌唇粘连术的。仅有 20 名带鼻饲管出院的婴儿中有 4 名需要使用 >2 周。内软腭裂成形术和腭裂闭合术分别在开始 PEBP 治疗 3 个月和 6 个月后进行。
在 RS 治疗中应用正畸器械尚未在全球范围内得到认可。我们希望我们关于 PEBP 的学习曲线和建议将有助于实施这种高效且非手术的治疗选择。