Lancet. 2017 May 13;389(10082):1885-1906. doi: 10.1016/S0140-6736(17)30819-X. Epub 2017 Apr 5.
The scale-up of tobacco control, especially after the adoption of the Framework Convention for Tobacco Control, is a major public health success story. Nonetheless, smoking remains a leading risk for early death and disability worldwide, and therefore continues to require sustained political commitment. The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) offers a robust platform through which global, regional, and national progress toward achieving smoking-related targets can be assessed.
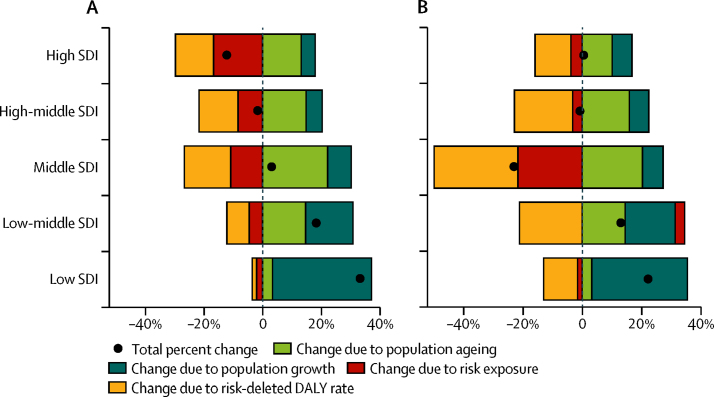
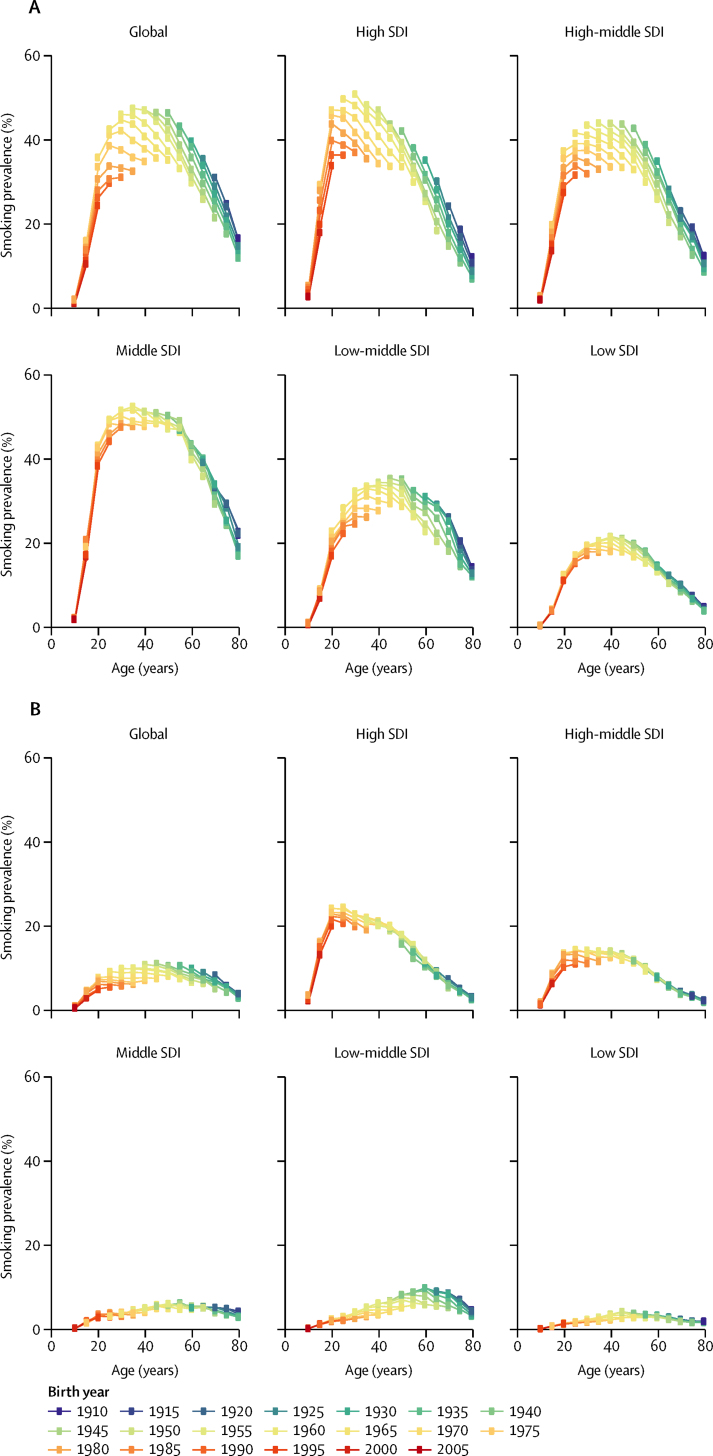
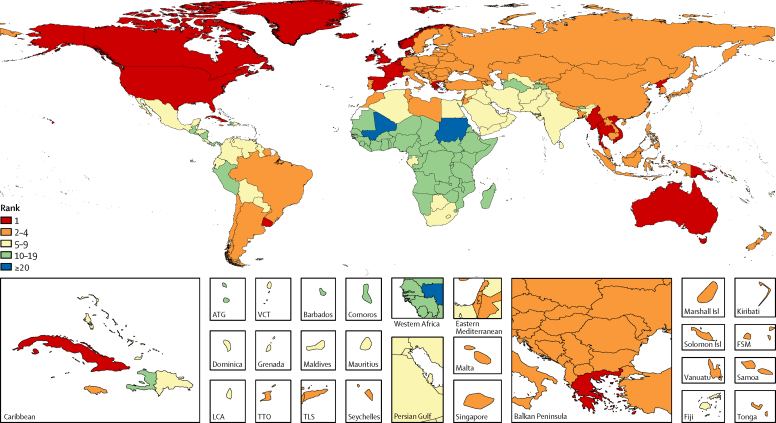
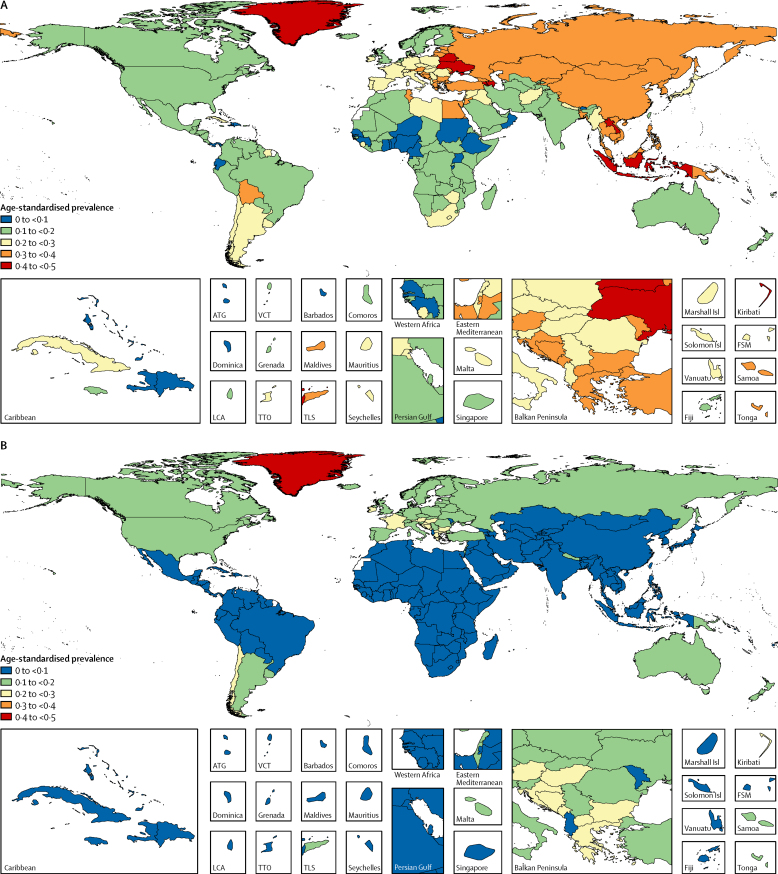
We synthesised 2818 data sources with spatiotemporal Gaussian process regression and produced estimates of daily smoking prevalence by sex, age group, and year for 195 countries and territories from 1990 to 2015. We analysed 38 risk-outcome pairs to generate estimates of smoking-attributable mortality and disease burden, as measured by disability-adjusted life-years (DALYs). We then performed a cohort analysis of smoking prevalence by birth-year cohort to better understand temporal age patterns in smoking. We also did a decomposition analysis, in which we parsed out changes in all-cause smoking-attributable DALYs due to changes in population growth, population ageing, smoking prevalence, and risk-deleted DALY rates. Finally, we explored results by level of development using the Socio-demographic Index (SDI).
Worldwide, the age-standardised prevalence of daily smoking was 25·0% (95% uncertainty interval [UI] 24·2-25·7) for men and 5·4% (5·1-5·7) for women, representing 28·4% (25·8-31·1) and 34·4% (29·4-38·6) reductions, respectively, since 1990. A greater percentage of countries and territories achieved significant annualised rates of decline in smoking prevalence from 1990 to 2005 than in between 2005 and 2015; however, only four countries had significant annualised increases in smoking prevalence between 2005 and 2015 (Congo [Brazzaville] and Azerbaijan for men and Kuwait and Timor-Leste for women). In 2015, 11·5% of global deaths (6·4 million [95% UI 5·7-7·0 million]) were attributable to smoking worldwide, of which 52·2% took place in four countries (China, India, the USA, and Russia). Smoking was ranked among the five leading risk factors by DALYs in 109 countries and territories in 2015, rising from 88 geographies in 1990. In terms of birth cohorts, male smoking prevalence followed similar age patterns across levels of SDI, whereas much more heterogeneity was found in age patterns for female smokers by level of development. While smoking prevalence and risk-deleted DALY rates mostly decreased by sex and SDI quintile, population growth, population ageing, or a combination of both, drove rises in overall smoking-attributable DALYs in low-SDI to middle-SDI geographies between 2005 and 2015.
The pace of progress in reducing smoking prevalence has been heterogeneous across geographies, development status, and sex, and as highlighted by more recent trends, maintaining past rates of decline should not be taken for granted, especially in women and in low-SDI to middle-SDI countries. Beyond the effect of the tobacco industry and societal mores, a crucial challenge facing tobacco control initiatives is that demographic forces are poised to heighten smoking's global toll, unless progress in preventing initiation and promoting cessation can be substantially accelerated. Greater success in tobacco control is possible but requires effective, comprehensive, and adequately implemented and enforced policies, which might in turn require global and national levels of political commitment beyond what has been achieved during the past 25 years.
Bill & Melinda Gates Foundation and Bloomberg Philanthropies.
烟草控制的扩大,特别是在《烟草控制框架公约》通过之后,是一项重大的公共卫生成功案例。尽管如此,吸烟仍然是导致全球早逝和残疾的主要风险因素,因此仍需要持续的政治承诺。全球疾病、伤害和风险因素研究(GBD)提供了一个强大的平台,可以通过该平台评估在实现与吸烟相关的目标方面取得的全球、区域和国家进展。
我们综合了 2818 个数据源,利用时空高斯过程回归,为 195 个国家和地区 1990 年至 2015 年的男女性别、年龄组和年份生成了每日吸烟流行率的估计值。我们分析了 38 个风险-结果对,以生成归因于吸烟的死亡率和疾病负担的估计值,以残疾调整生命年(DALY)衡量。然后,我们对出生年份队列的吸烟流行率进行了队列分析,以更好地了解吸烟的时间年龄模式。我们还进行了分解分析,在该分析中,我们将由于人口增长、人口老龄化、吸烟流行率和风险消除 DALY 率变化而导致的全因归因于吸烟的 DALY 变化分解开来。最后,我们使用社会人口指数(SDI)探索了不同发展水平的结果。
全球范围内,男性的年龄标准化日吸烟率为 25.0%(95%不确定性区间[UI]24.2-25.7),女性为 5.4%(5.1-5.7),分别比 1990 年下降了 28.4%(25.8-31.1)和 34.4%(29.4-38.6)。自 1990 年以来,与 2005 年至 2015 年相比,更多的国家和地区实现了吸烟流行率的年化显著下降率;然而,只有四个国家的吸烟流行率在 2005 年至 2015 年期间出现了显著的年化上升(男性为刚果(布)和阿塞拜疆,女性为科威特和东帝汶)。2015 年,全球 11.5%的死亡(640 万[95% UI 570 万至 700 万])归因于全球吸烟,其中 52.2%发生在四个国家(中国、印度、美国和俄罗斯)。吸烟在 2015 年 109 个国家和地区的疾病负担中被列为五个主要风险因素之一,高于 1990 年的 88 个地区。就出生队列而言,男性吸烟流行率在不同的 SDI 水平上遵循相似的年龄模式,而女性吸烟者的年龄模式在发展水平上则存在更多的异质性。尽管吸烟流行率和风险消除 DALY 率主要按性别和 SDI 五分位数下降,但在 2005 年至 2015 年期间,人口增长、人口老龄化或两者的结合导致低 SDI 至中 SDI 地区的全因归因于吸烟的 DALY 增加。
在减少吸烟流行率方面,各地、各发展水平和各性别之间的进展速度存在差异,正如最近的趋势所强调的那样,不应理所当然地认为过去的下降速度会保持下去,尤其是在女性和低 SDI 至中 SDI 国家。除了烟草业和社会习俗的影响之外,烟草控制倡议面临的一个关键挑战是,除非在预防开始吸烟和促进戒烟方面取得实质性进展,否则人口趋势可能会加剧吸烟对全球的影响。但更成功的烟草控制是有可能的,但需要有效的、全面的、充分实施和执行的政策,这可能反过来需要在全球和国家层面上达到过去 25 年来所取得的政治承诺水平。
比尔和梅琳达·盖茨基金会和彭博慈善基金会。