Sato Shinri, Shinoda Hajime, Nagai Norihiro, Suzuki Misa, Uchida Atsuro, Kurihara Toshihide, Kamoshita Mamoru, Tomita Yohei, Iyama Chigusa, Minami Sakiko, Yuki Kenya, Tsubota Kazuo, Ozawa Yoko
aDepartment of Ophthalmology bLaboratory of Retinal Cell Biology, Keio University, School of Medicine, Tokyo, Japan.
Medicine (Baltimore). 2017 Apr;96(16):e6459. doi: 10.1097/MD.0000000000006459.
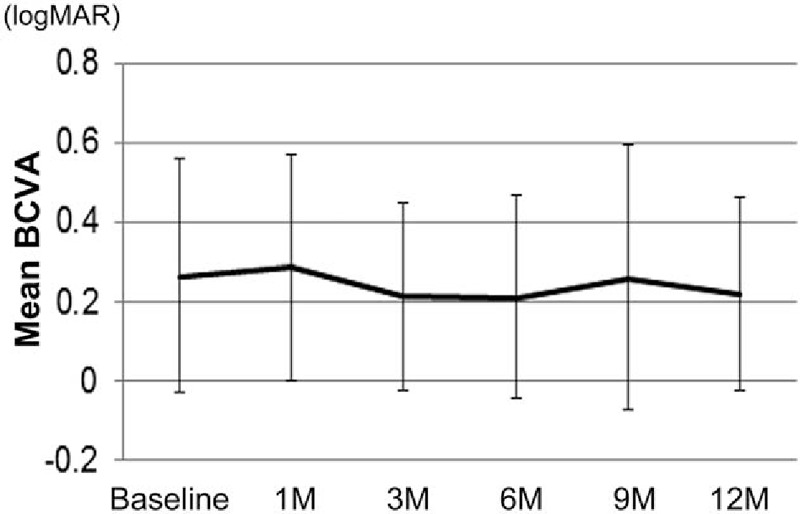
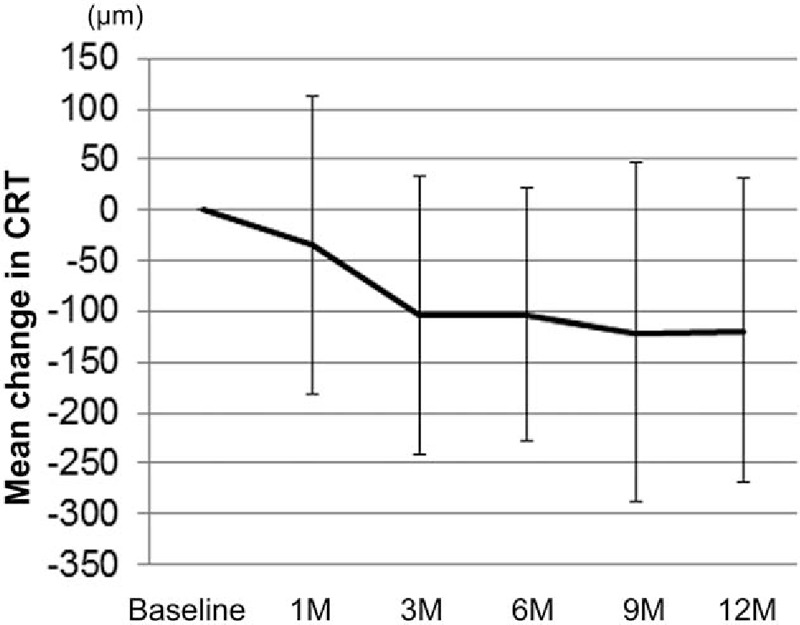
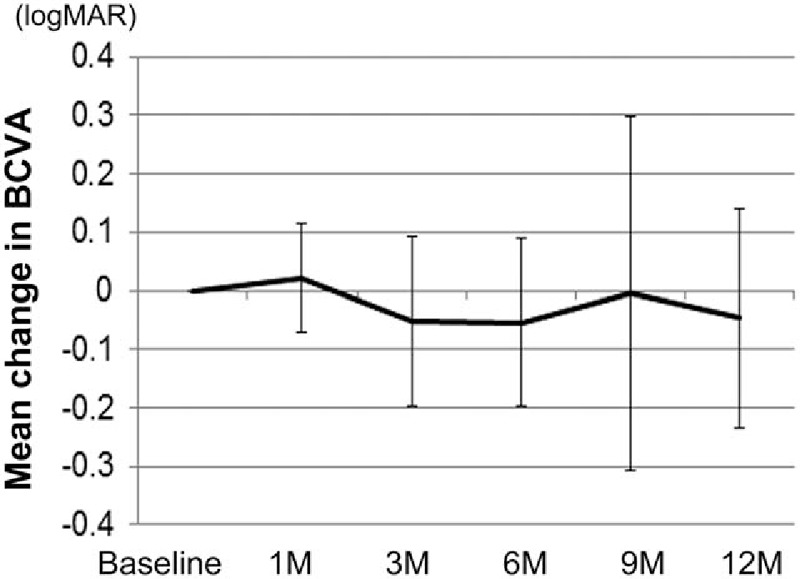
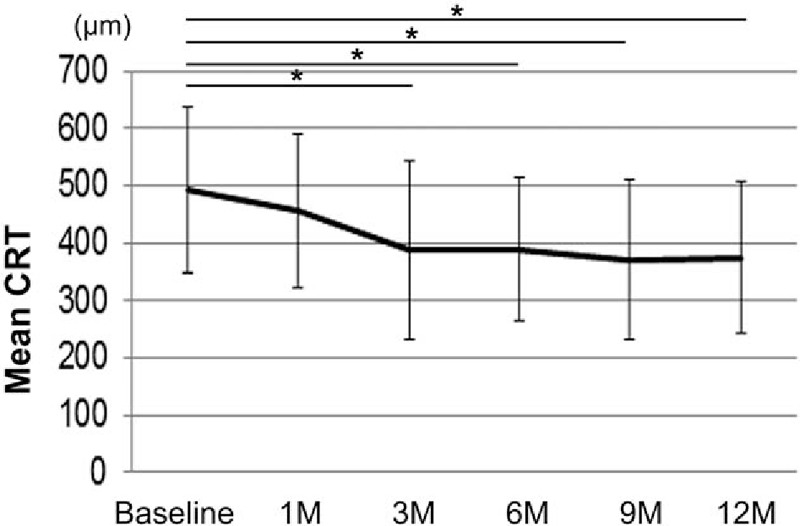
Intravitreal ranibizumab (IVR) has been approved for treating diabetic macular edema (DME), and is used in daily clinical practice. However, the treatment efficacies of IVR monotherapy in real-world clinical settings are not well known.The medical records of 56 eyes from 38 patients who received their first IVR for DME between April 2014 and March 2015, and were retreated with IVR monotherapy as needed with no rescue treatment, such as laser photocoagulation, were retrospectively reviewed. The clinical course, best-corrected visual acuity (BCVA), and fundus findings at baseline, before the initial IVR injection, and at 12 months, were evaluated.Twenty-five eyes from 25 patients (16 men; mean age 68.7 ± 9.8 years) who received IVR in the first eye, or unilaterally, without any other treatments during follow-up were included. After 12 months, mean central retinal thickness (CRT), which includes edema, was reduced (P = .003), although mean BCVA remained unchanged. There was a negative correlation between individual changes in BCVA (r = -0.57; P = .003) and CRT (r = -0.60; P = .002) at 12 months compared with baseline values. BCVA changes were greater in individuals with a history of pan-retinal photocoagulation at baseline (P = .026). After adjusting for age and sex, CRT improvement >100 μm at 12 months was associated with a greater CRT at baseline (OR 0.87 per 10 μm [95% CI 0.72-0.97]; P = .018) according to logistic regression analyses; however, better BCVA and CRT at 12 months were associated with a better BCVA (r = 0.77; P < .001) and lower CRT (r = 0.41; P = .039) at baseline, respectively, according to linear regression analyses.IVR monotherapy suppressed DME, and the effects varied according to baseline conditions. Eyes that had poorer BCVA or greater CRT, or a history of pan-retinal photocoagulation at baseline, demonstrated greater improvement with IVR monotherapy. In contrast, to achieve better outcome values, DME eyes should be treated before the BCVA and CRT deteriorate. These findings advance our understanding of the optimal use of IVR for DME in daily clinical practice, although further study is warranted.
玻璃体内注射雷珠单抗(IVR)已被批准用于治疗糖尿病性黄斑水肿(DME),并应用于日常临床实践。然而,IVR单药治疗在实际临床环境中的治疗效果尚不清楚。回顾性分析了2014年4月至2015年3月期间38例首次接受IVR治疗DME的患者的56只眼的病历,这些患者在需要时接受IVR单药再次治疗,未接受激光光凝等挽救治疗。评估了临床病程、最佳矫正视力(BCVA)以及基线、首次IVR注射前和12个月时的眼底检查结果。纳入了25例患者的25只眼(16例男性;平均年龄68.7±9.8岁),这些患者第一眼接受IVR治疗,或单侧接受IVR治疗,随访期间未接受任何其他治疗。12个月后,包括水肿在内的平均中心视网膜厚度(CRT)降低(P = 0.003),尽管平均BCVA保持不变。与基线值相比,12个月时个体BCVA变化(r = -0.57;P = 0.003)和CRT变化(r = -0.60;P = 0.002)之间呈负相关。基线时有全视网膜光凝病史的个体BCVA变化更大(P = 0.026)。根据逻辑回归分析,在调整年龄和性别后,12个月时CRT改善>100μm与基线时CRT更高相关(每10μm的OR为0.87 [95%CI 0.72 - 0.97];P = 0.018);然而,根据线性回归分析,12个月时更好的BCVA和CRT分别与基线时更好的BCVA(r = 0.77;P < 0.001)和更低的CRT(r = 0.41;P = 0.039)相关。IVR单药治疗可抑制DME,其效果因基线情况而异。基线时BCVA较差或CRT较高或有全视网膜光凝病史的眼,IVR单药治疗显示出更大的改善。相比之下,为了获得更好的结果值,DME眼应在BCVA和CRT恶化之前进行治疗。这些发现增进了我们对IVR在日常临床实践中治疗DME的最佳应用的理解,尽管仍需进一步研究。