Suárez-Llanos José Pablo, Benítez-Brito Néstor, Vallejo-Torres Laura, Delgado-Brito Irina, Rosat-Rodrigo Adriá, Hernández-Carballo Carolina, Ramallo-Fariña Yolanda, Pereyra-García-Castro Francisca, Carlos-Romero Juan, Felipe-Pérez Nieves, García-Niebla Jennifer, Calderón-Ledezma Eduardo Mauricio, González-Melián Teresa de Jesús, Llorente-Gómez de Segura Ignacio, Barrera-Gómez Manuel Ángel
Endocrinology and Nutrition Department, Hospital Universitario Nuestra Señora de Candelaria, Ctra. Del Rosario 145, Santa Cruz de Tenerife, 38010, Spain.
Canary Foundation for Health Research (FUNCANIS) Evaluation Service of the Canary Health System (SESCS), Research Network on Health Services Chronic Disease (REDISSEC), Canary Center for Biomedical Research (CIBICAN), Santa Cruz de Tenerife, Spain.
BMC Health Serv Res. 2017 Apr 20;17(1):292. doi: 10.1186/s12913-017-2218-z.
Malnutrition is highly prevalent in hospitalized patients and results in a worsened clinical course as well as an increased length of stay, mortality, and costs. Therefore, simple nutrition screening systems, such as CIPA (control of food intake, protein, anthropometry), may be implemented to facilitate the patient's recovery process. The aim of this study is to evaluate the effectiveness and cost-effectiveness of implementing such screening tool in a tertiary hospital, consistent with the lack of similar, published studies on any hospital nutrition screening system.
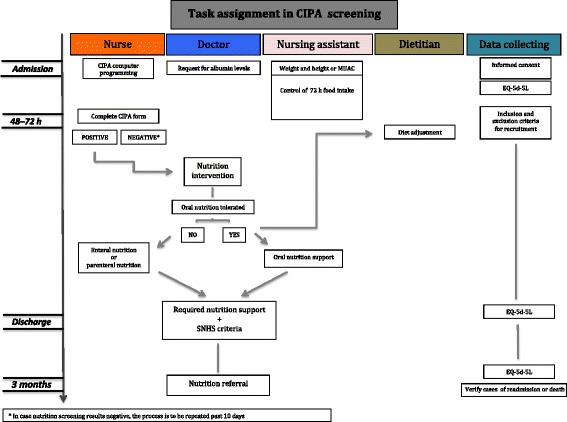
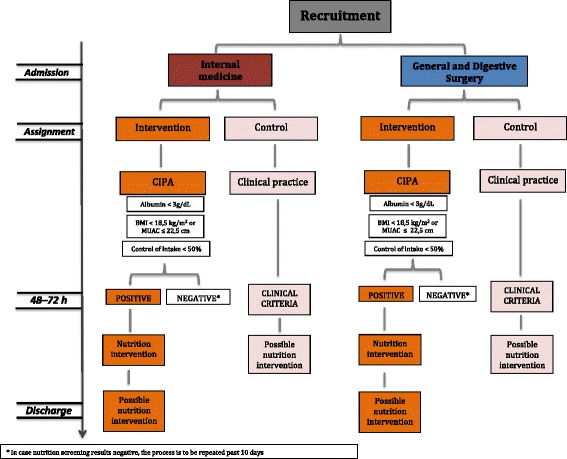
The present study is carried out as an open, controlled, randomized study on patients that were admitted to the Internal Medicine and the General and Digestive Surgery ward; the patients were randomized to either a control or an intervention group (n = 824, thereof 412 patients in each of the two study arms). The control group underwent usual inpatient clinical care, while the intervention group was evaluated with the CIPA screening tool for early detection of malnutrition and treated accordingly. CIPA nutrition screening was performed upon hospital admission and classified positive when at least one of the following parameters was met: 72 h food intake control < 50%, serum albumin < 3 g/dL, body mass index < 18.5 kg/m (or mid-upper arm circumference ≤ 22.5 cm). In this case, the doctor decided on whether or not providing nutrition support. The following variables will be evaluated: hospital length of stay (primary endpoint), mortality, 3-month readmission, and in-hospital complications. Likewise, the quality of life questionnaires EQ-5D-5 L are being collected for all patients at hospital admission, discharge, and 3 months post-discharge. Analysis of cost-effectiveness will be performed by measuring effectiveness in terms of quality-adjusted life years (QALYs). The cost per patient will be established by identifying health care resource utilization; cost-effectiveness will be determined through the incremental cost-effectiveness ratio (ICER). We will calculate the incremental cost per QALY gained with respect to the intervention.
This ongoing trial aims to evaluate the cost-effectiveness of implementing the malnutrition screening tool CIPA in a tertiary hospital.
Clinical Trial.gov ( NCT02721706 ). First receivevd: March 1, 2016 Last updated: April 8, 2017 Last verified: April 2017.
营养不良在住院患者中非常普遍,会导致临床病程恶化,住院时间延长、死亡率增加以及成本上升。因此,可以实施简单的营养筛查系统,如CIPA(食物摄入量、蛋白质、人体测量控制),以促进患者的康复进程。本研究的目的是评估在一家三级医院实施这种筛查工具的有效性和成本效益,因为目前缺乏关于任何医院营养筛查系统的类似已发表研究。
本研究作为一项开放性、对照、随机研究,对内科、普通外科和消化外科病房收治的患者进行;患者被随机分为对照组或干预组(n = 824,两个研究组各412例患者)。对照组接受常规住院临床护理,而干预组使用CIPA筛查工具进行评估,以早期发现营养不良并相应进行治疗。入院时进行CIPA营养筛查,当满足以下至少一项参数时分类为阳性:72小时食物摄入量控制<50%、血清白蛋白<3 g/dL、体重指数<18.5 kg/m²(或上臂中部周长≤22.5 cm)。在这种情况下,由医生决定是否提供营养支持。将评估以下变量:住院时间(主要终点)、死亡率、3个月再入院率和院内并发症。同样,在入院、出院时以及出院后3个月为所有患者收集生活质量问卷EQ-5D-5L。将通过以质量调整生命年(QALY)衡量有效性来进行成本效益分析。通过确定医疗资源利用情况来确定每位患者的成本;将通过增量成本效益比(ICER)来确定成本效益。我们将计算相对于干预措施每获得一个QALY的增量成本。
这项正在进行的试验旨在评估在一家三级医院实施营养不良筛查工具CIPA的成本效益。
ClinicalTrial.gov(NCT02721706)。首次接收日期:2016年3月1日。最后更新日期:2017年4月8日。最后核实日期:2017年4月。