Cassidy Sophie, Chau Josephine Y, Catt Michael, Bauman Adrian, Trenell Michael I
Institute of Cellular Medicine, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, NE2 4HH, UK.
Prevention Research Collaboration, Sydney School of Public Health, Charles Perkins Centre D17, Level 6 The Hub, University of Sydney, Sydney, NSW, 2006, Australia.
Int J Behav Nutr Phys Act. 2017 Apr 28;14(1):57. doi: 10.1186/s12966-017-0514-y.
An unhealthy lifestyle is one of the greatest contributors to obesity. A number of behaviours are linked with obesity, but are often measured separately. The UK Biobank cohort of >500,000 participants allows us to explore these behaviours simultaneously. We therefore aimed to compare physical activity, television (TV) viewing and sleep duration across body mass index (BMI) categories in a large sample of UK adults.
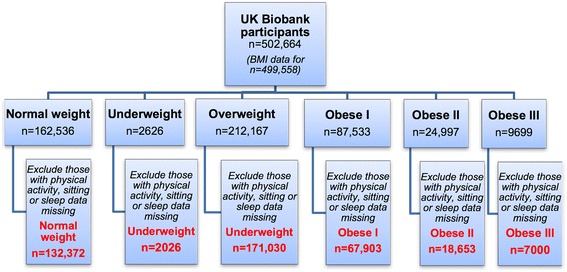
UK Biobank participants were recruited and baseline measures were taken between 2007 and 2010 and data analysis was performed in 2015. BMI was measured objectively using trained staff. Self-report questionnaires were used to measure lifestyle behaviours including the international physical activity questionnaire (IPAQ-short form) for physical activity. During data analysis, six groups were defined based on BMI; 'Underweight' (n = 2026), 'Normal weight' (n = 132,372), 'Overweight (n = 171,030), 'Obese I' (n = 67,903), 'Obese II' (n = 18,653) and 'Obese III' (n = 7000). The odds of reporting unhealthy lifestyle behaviours (low physical activity, high TV viewing or poor sleep duration) were compared across BMI groups using logistic regression analysis.
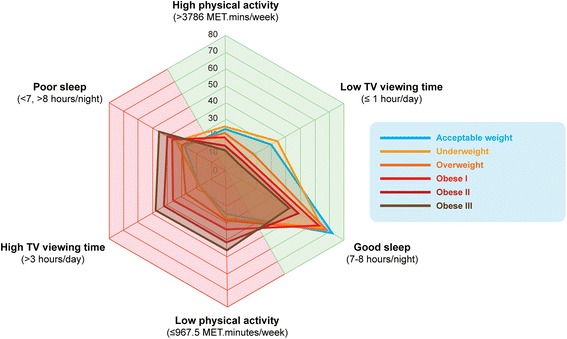
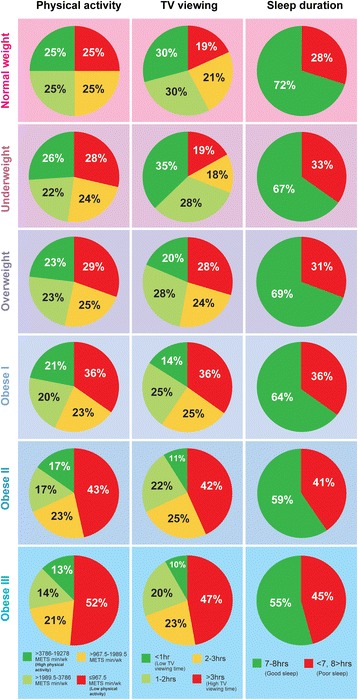
Overweight and obese adults were more likely to report low levels of physical activity (≤967.5 MET.mins/wk) ('Overweight'-OR [95% CI]: 1.23 [1.20 to 1.26], 'Obese I' 1.66 [1.61-1.71], 'Obese II' 2.21 [2.12-2.30], and 'Obese III' 3.13 [2.95 to 3.23]) compared to 'Normal weight' adults. The odds of reporting high TV viewing (3 h/day) was greater in 'Overweight' (1.52 [1.48 to 1.55]) and obese adults ('Obese I' 2.06 [2.00-2.12], 'Obese II' 2.69 [2.58-2.80], 'Obese III' 3.26 [3.07 to 3.47]), and poor sleep duration (<7, >8 h/night) was higher in 'Overweight' (1.09 [1.07 to 1.12]) and obese adults ('Obese I' 1.31 [1.27-1.34], 'Obese II' 1.50 [1.44-1.56], 'Obese III' (1.78 [1.68 to 1.89]) compared to the 'Normal weight' group. These lifestyle behaviours were clustered, the odds of reporting simultaneous low physical activity, high TV viewing and poor sleep (unhealthy behavioural phenotype) was higher than reporting these behaviours independently, in overweight and obese groups. 'Obese III' adults were almost six times more likely (5.47 [4.96 to 6.05]) to report an unhealthy behavioural phenotype compared to the 'Normal weight' group.
Overweight and obese adults report low levels of physical activity, high TV viewing and poor sleep duration. These behaviours seem to cluster and collectively expose individuals to greater risk of obesity. Multiple lifestyle behaviours should be targeted in future interventions.
不健康的生活方式是导致肥胖的最大因素之一。许多行为都与肥胖有关,但通常是单独进行测量的。英国生物银行拥有超过50万名参与者的队列,这使我们能够同时探究这些行为。因此,我们旨在比较英国大量成年人中不同体重指数(BMI)类别之间的身体活动、看电视(TV)时间和睡眠时间。
英国生物银行的参与者于2007年至2010年期间招募并进行了基线测量,并于2015年进行了数据分析。BMI由经过培训的工作人员客观测量。使用自我报告问卷来测量生活方式行为,包括用于身体活动的国际身体活动问卷(IPAQ简表)。在数据分析过程中,根据BMI定义了六组;“体重过轻”(n = 2026)、“正常体重”(n = 132372)、“超重”(n = 171030)、“肥胖I级”(n = 67903)、“肥胖II级”(n = 18653)和“肥胖III级”(n = 7000)。使用逻辑回归分析比较不同BMI组报告不健康生活方式行为(低身体活动、高看电视时间或睡眠时间不佳)的几率。
与“正常体重”的成年人相比,超重和肥胖的成年人更有可能报告低水平的身体活动(≤967.5代谢当量·分钟/周)(“超重”-比值比[95%置信区间]:1.23[1.20至1.26],“肥胖I级”1.66[1.61 - 1.71],“肥胖II级”2.21[2.12 - 2.30],“肥胖III级”3.13[2.95至3.23])。报告高看电视时间(每天3小时)的几率在“超重”人群中更高(1.52[1.48至1.55]),在肥胖成年人中也更高(“肥胖I级”2.06[2.00 - 2.12],“肥胖II级”2.69[2.58 - 2.80],“肥胖III级”3.26[3.07至3.47]),并且睡眠时间不佳(<7小时、>8小时/晚)在“超重”人群中更高(1.09[1.07至1.12]),在肥胖成年人中也更高(“肥胖I级”1.31[1.27 - 1.34],“肥胖II级”1.50[1.44 - 1.56],“肥胖III级”1.78[1.68至1.89]),与“正常体重”组相比。这些生活方式行为是聚集出现的,在超重和肥胖组中,报告同时存在低身体活动、高看电视时间和睡眠不佳(不健康行为表型)的几率高于单独报告这些行为的几率。与“正常体重”组相比,“肥胖III级”的成年人报告不健康行为表型的可能性几乎高出六倍(5.47[4.96至6.05])。
超重和肥胖的成年人报告身体活动水平低、看电视时间长和睡眠时间不佳。这些行为似乎会聚集在一起,使个体面临更高的肥胖风险。在未来的干预措施中应针对多种生活方式行为。