Makam Anil N, Nguyen Oanh K, Clark Christopher, Halm Ethan A
Division of General Internal Medicine, University of Texas Southwestern Medical Center, Dallas, TX; Division of Outcomes and Health Services Research, University of Texas Southwestern Medical Center, Dallas, TX.
Office of Research Administration, Parkland Health and Hospital System, Dallas, TX.
J Hosp Med. 2017 May;12(5):317-322. doi: 10.12788/jhm.2712.
Although hypothesized to be a hazard of hospitalization, it is unclear whether hospital-acquired anemia (HAA) is associated with increased adverse outcomes following discharge.
To examine the incidence, predictors, and postdischarge outcomes associated with HAA.
Observational cohort study using electronic health record data.
Consecutive medicine discharges between November 1, 2009 and October 30, 2010 from 6 Texas hospitals, including safety-net, teaching, and nonteaching sites. Patients with anemia on admission or missing hematocrit values at admission or discharge were excluded.
HAA was defined using the last hematocrit value prior to discharge and categorized by severity. The primary outcome was a composite of 30-day mortality and nonelective readmission.
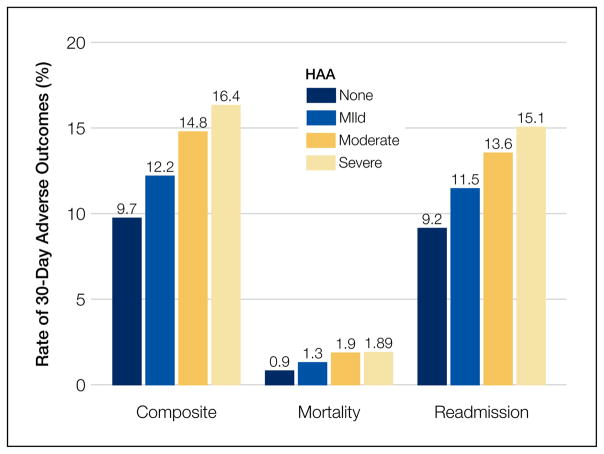
Among 11,309 patients, one-third developed HAA (21.6% with mild HAA; 10.1% with moderate HAA; and 1.4% with severe HAA). The 2 strongest potentially modifiable predictors of developing moderate or severe HAA were length of stay (adjusted odds ratio [OR], 1.26 per day; 95% confidence interval [CI], 1.23-1.29) and receipt of a major procedure (adjusted OR, 5.09; 95% CI, 3.79-6.82). Patients without HAA had a 9.7% incidence for the composite outcome versus 16.4% for those with severe HAA. Severe HAA was independently associated with a 39% increase in the odds for 30-day readmission or death (95% CI, 1.09-1.78). Most patients with severe HAA (85%) underwent a major procedure, had a discharge diagnosis of hemorrhage, and/or a discharge diagnosis of hemorrhagic disorder.
Severe HAA is associated with increased odds for 30-day mortality and readmission after discharge; however, it is uncertain whether severe HAA is preventable. Journal of Hospital Medicine 2017;12:317-322.
尽管住院被认为是一种危险因素,但尚不清楚医院获得性贫血(HAA)是否与出院后不良结局增加相关。
研究HAA的发生率、预测因素及出院后结局。
使用电子健康记录数据的观察性队列研究。
2009年11月1日至2010年10月30日期间,来自德克萨斯州6家医院(包括安全网医院、教学医院和非教学医院)的连续内科出院患者。排除入院时贫血或入院或出院时血细胞比容值缺失的患者。
HAA根据出院前最后一次血细胞比容值定义,并按严重程度分类。主要结局是30天死亡率和非选择性再入院的综合指标。
在11309例患者中,三分之一发生了HAA(轻度HAA占21.6%;中度HAA占10.1%;重度HAA占1.4%)。发生中度或重度HAA的两个最强的潜在可改变预测因素是住院时间(调整后的优势比[OR],每天1.26;95%置信区间[CI],1.23 - 1.29)和接受大手术(调整后的OR,5.09;95%CI,3.79 - 6.82)。无HAA的患者综合结局发生率为9.7%,而重度HAA患者为16.4%。重度HAA与30天再入院或死亡几率增加39%独立相关(95%CI,1.09 - 1.78)。大多数重度HAA患者(85%)接受了大手术,出院诊断为出血和/或出血性疾病。
重度HAA与出院后30天死亡率和再入院几率增加相关;然而,重度HAA是否可预防尚不确定。《医院医学杂志》2017年;12:317 - 322。