Bruce Marino A, Martins David, Duru Kenrik, Beech Bettina M, Sims Mario, Harawa Nina, Vargas Roberto, Kermah Dulcie, Nicholas Susanne B, Brown Arleen, Norris Keith C
Center for Research on Men's Health, Vanderbilt University, Nashville, Tennessee, United States of America.
Department of Internal Medicine, Charles R. Drew University School of Medicine and Science, Los Angeles, California, United States of America.
PLoS One. 2017 May 16;12(5):e0177618. doi: 10.1371/journal.pone.0177618. eCollection 2017.
Religiosity has been associated with positive health outcomes. Hypothesized pathways for this association include religious practices, such as church attendance, that result in reduced stress.
The objective of this study was to examine the relationship between religiosity (church attendance), allostatic load (AL) (a physiologic measure of stress) and all-cause mortality in middle-aged adults.
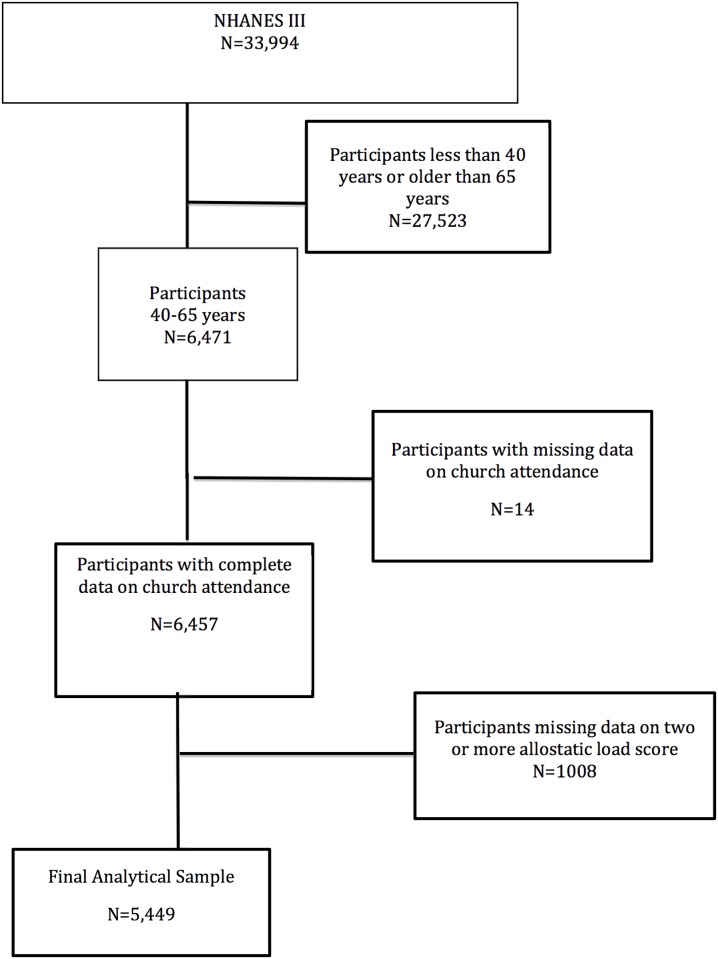
DESIGN, SETTING AND PARTICIPANTS: Data for this study are from NHANES III (1988-1994). The analytic sample (n = 5449) was restricted to adult participants, who were between 40-65 years of age at the time of interview, had values for at least 9 out of 10 clinical/biologic markers used to derive AL, and had complete information on church attendance.
The primary outcomes were AL and mortality. AL was derived from values for metabolic, cardiovascular, and nutritional/inflammatory clinical/biologic markers. Mortality was derived from a probabilistic algorithm matching the NHANES III Linked Mortality File to the National Death Index through December 31, 2006, providing up to 18 years follow-up. The primary predictor variable was baseline report of church attendance over the past 12 months. Cox proportional hazard logistic regression models contained key covariates including socioeconomic status, self-rated health, co-morbid medical conditions, social support, healthy eating, physical activity, and alcohol intake.
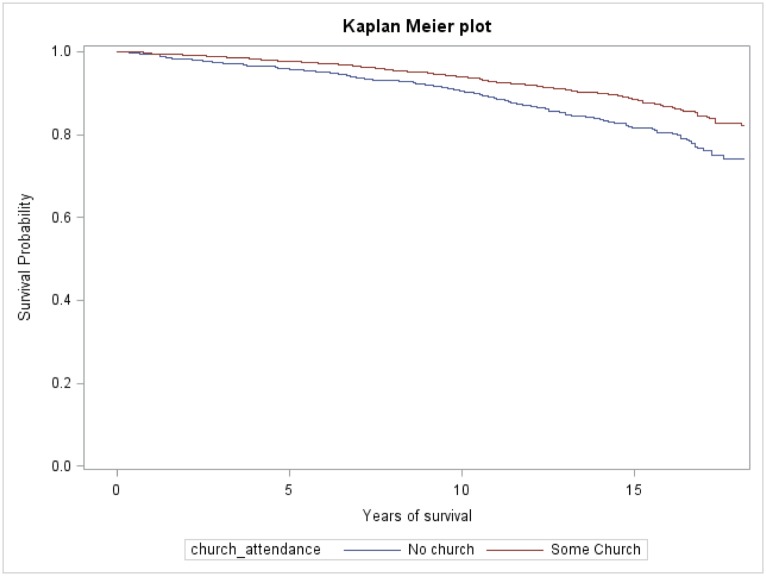
Churchgoers (at least once a year) comprised 64.0% of the study cohort (n = 3782). Non-churchgoers had significantly higher overall mean AL scores and higher prevalence of high-risk values for 3 of the 10 markers of AL than did churchgoers. In bivariate analyses non-churchgoers, compared to churchgoers, had higher odds of an AL score 2-3 (OR 1.24; 95% CI 1.01, 1.50) or ≥4 (OR 1.38; 95% CI 1.11, 1.71) compared to AL score of 0-1. More frequent churchgoers (more than once a week) had a 55% reduction of all-cause mortality risk compared with non-churchgoers. (HR 0.45, CI 0.24-0.85) in the fully adjusted model that included AL.
We found a significant association between church attendance and mortality among middle-aged adults after full adjustments. AL, a measure of stress, only partially explained differences in mortality between church and non-church attendees. These findings suggest a potential independent effect of church attendance on mortality.
宗教虔诚度与积极的健康结果相关。这种关联的假设途径包括宗教活动,如参加教会,从而减轻压力。
本研究的目的是检验宗教虔诚度(参加教会情况)、应激负荷(AL)(一种压力的生理指标)与中年成年人全因死亡率之间的关系。
设计、背景和参与者:本研究的数据来自美国国家健康和营养检查调查III(NHANES III,1988 - 1994年)。分析样本(n = 5449)仅限于成年参与者,他们在访谈时年龄在40 - 65岁之间,用于计算AL的10项临床/生物学指标中至少有9项有数据,且有关于参加教会情况的完整信息。
主要结局是AL和死亡率。AL由代谢、心血管以及营养/炎症方面的临床/生物学指标值得出。死亡率通过一种概率算法得出,该算法将NHANES III关联死亡率文件与截至2006年12月31日的国家死亡指数进行匹配,提供长达18年的随访。主要预测变量是过去12个月参加教会情况的基线报告。Cox比例风险逻辑回归模型包含关键协变量,包括社会经济地位、自我评估健康状况、合并症、社会支持、健康饮食、体育活动和酒精摄入量。
经常去教堂的人(至少每年一次)占研究队列的64.0%(n = 3782)。与经常去教堂的人相比,不常去教堂的人总体平均AL得分显著更高,在用于计算AL的10项指标中的3项上,高风险值的患病率也更高。在二元分析中,与经常去教堂的人相比,不常去教堂的人AL得分在2 - 3(OR 1.24;95% CI 1.01,1.50)或≥4(OR 1.38;95% CI 1.11,1.71)的几率高于AL得分为0 - 1的情况。与不常去教堂的人相比,更频繁去教堂的人(每周不止一次)全因死亡风险降低了55%。(在包含AL的完全调整模型中,HR 0.45,CI 0.24 - 0.85)
在进行全面调整后,我们发现中年成年人中参加教会情况与死亡率之间存在显著关联。AL作为一种压力指标,仅部分解释了去教堂和不去教堂的人在死亡率上的差异。这些发现表明参加教会对死亡率可能有独立的潜在影响。