Gudbrandsson Birgir, Molberg Øyvind, Palm Øyvind
Oslo University Hospital, Postboks 4950 Nydalen, 0424, Oslo, Norway.
Department of Rheumatology, Oslo University Hospital - Rikshospitalet, Oslo, Norway.
Arthritis Res Ther. 2017 May 18;19(1):99. doi: 10.1186/s13075-017-1316-y.
Magnetic resonance imaging (MRI) and computed tomography (CT) angiography have now largely replaced interventional angiography in the diagnoses and follow up of Takayasu arteritis (TAK) but data on the effects of this change of imaging method on diagnostic delay and vascular damage, and detailed data on the effect of different treatment regimens on the accumulation of vascular damage are missing. The aim of this study was to assess time trends in diagnostic delay, therapeutic approaches, arterial lesion accrual, persistent disease activity and remission rates in TAK.
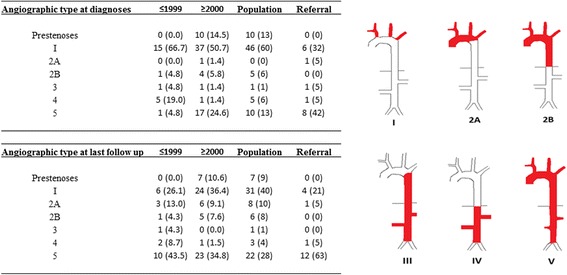
The study cohort included all 78 patients from the 1999 - 2012 population-based South-East Norway TAK cohort and 19 patients from a tertiary referral cohort. TAK was classified by the 1990 American College of Rheumatology criteria and/or the 1995 modified Ishikawa diagnostic criteria. Data were retrieved by review of electronic patient journals and imaging data analyses.
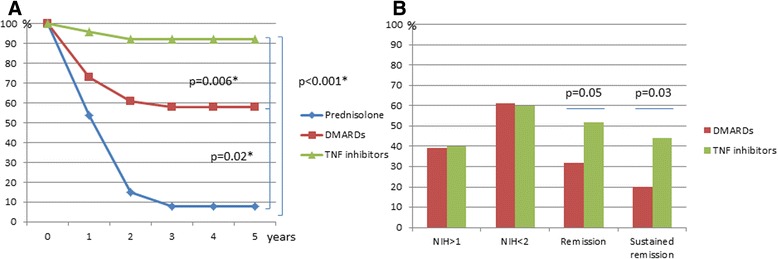
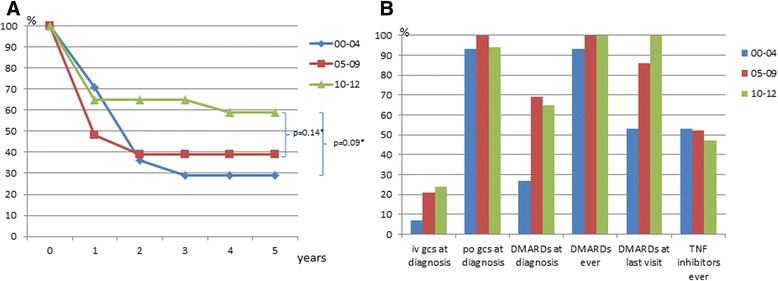
Diagnostic delay fell significantly during the study period and the number of lesions at diagnoses fell from three to two. Patients diagnosed from 2000 onwards more often received up-front treatment with disease-modifying antirheumatic drugs (DMARDs) than those diagnosed before 2000 (51% vs 4%; p < 0.01), and they were more often treated with TNF inhibitors during the disease course (44% vs 14%). During the first 2 years after initiation of therapy, 10% (3/32) of TNF-inhibitor-treated patients developed new lesions, compared to 40% (16/40) on DMARD treatment (OR 0.13) and 92% (14/15) on prednisolone monotherapy (OR 0.02). Patients on TNF inhibitors had a higher sustained remission rate than patients on DMARDs (42% vs 20%; p = 0.03). From 2000 onwards, the proportion of patients without new arterial lesions during the first 5 years after diagnosis increased from 29% in the patients diagnosed in 2000-2004, to 39% in 2005-2009 and 59% of patients diagnosed in 2010-2012.
Our observational data indicate that more aggressive use of TNF inhibitors and DMARDs improve the outcome in TAK, but damage accrual is a continuous challenge and sustained remission is still relatively rare.
在大动脉炎(TAK)的诊断和随访中,磁共振成像(MRI)和计算机断层扫描(CT)血管造影现已在很大程度上取代了介入血管造影,但关于这种成像方法的改变对诊断延迟和血管损伤的影响的数据,以及关于不同治疗方案对血管损伤累积影响的详细数据尚缺。本研究的目的是评估TAK患者在诊断延迟、治疗方法、动脉病变累积、持续疾病活动和缓解率方面的时间趋势。
研究队列包括1999年至2012年基于挪威东南部人群的TAK队列中的所有78例患者以及来自三级转诊队列的19例患者。TAK根据1990年美国风湿病学会标准和/或1995年改良的石川诊断标准进行分类。通过查阅电子病历和影像学数据分析获取数据。
在研究期间,诊断延迟显著缩短,诊断时的病变数量从三个降至两个。2000年以后诊断的患者比2000年以前诊断的患者更常接受改善病情抗风湿药物(DMARDs)的初始治疗(51%对4%;p<0.01),并且在病程中接受肿瘤坏死因子(TNF)抑制剂治疗的频率更高(44%对14%)。在开始治疗后的前2年,接受TNF抑制剂治疗的患者中有10%(3/32)出现新病变,而接受DMARD治疗的患者中这一比例为40%(16/40)(比值比[OR]0.13),接受泼尼松龙单药治疗的患者中这一比例为92%(14/15)(OR 0.02)。接受TNF抑制剂治疗的患者持续缓解率高于接受DMARDs治疗的患者(42%对20%;p=0.03)。从2000年起,诊断后前5年无新动脉病变的患者比例从2000 - 2004年诊断的患者中的29%,增加到2005 - 2009年的39%以及2010 - 2012年诊断的患者中的59%。
我们的观察数据表明,更积极地使用TNF抑制剂和DMARDs可改善TAK的预后,但损伤累积仍是一个持续的挑战,持续缓解仍然相对少见。