Slogrove Amy L, Mahy Mary, Armstrong Alice, Davies Mary-Ann
Centre for Infectious Disease Epidemiology and Research, School of Public Health and Family Medicine, Faculty of Health Sciences, University of Cape Town, Cape Town, South Africa.
Strategic Information and Monitoring Division, UNAIDS, Geneva, Switzerland.
J Int AIDS Soc. 2017 May 16;20(Suppl 3):21520. doi: 10.7448/IAS.20.4.21520.
With increasing survival of vertically HIV-infected children and ongoing new horizontal HIV infections, the population of adolescents (age 10-19 years) living with HIV is increasing. This review aims to describe the epidemiology of the adolescent HIV epidemic and the ability of national monitoring systems to measure outcomes in HIV-infected adolescents through the adolescent transition to adulthood.
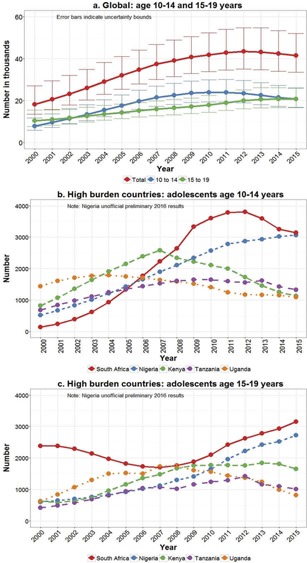
Differences in global trends between younger (age 10-14 years) and older (age 15-19 years) adolescents in key epidemic indicators are interrogated using 2016 UNAIDS estimates. National population-based survey data in the 15 highest adolescent HIV burden countries are evaluated and examples of national case-based surveillance systems described. Finally, we consider the potential impact of adolescent-specific recommendations in the 2016 WHO Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection.
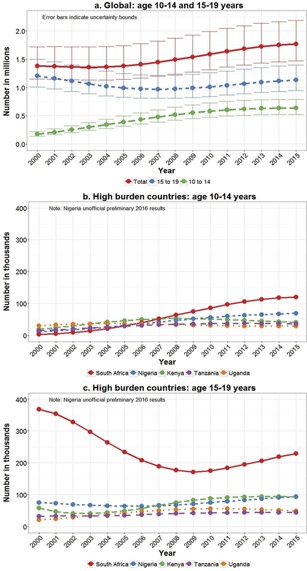
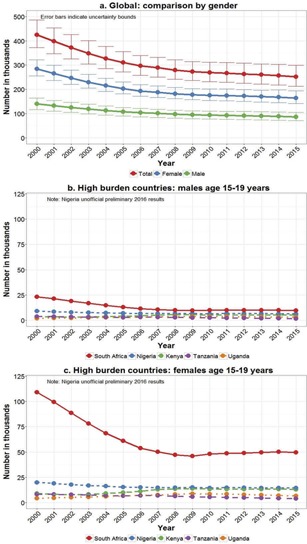
UNAIDS estimates indicate the population of adolescents living with HIV is increasing, new HIV infections in older adolescents are declining, and while AIDS-related deaths are beginning to decline in younger adolescents, they are still increasing in older adolescents. National population-based surveys provide valuable estimates of HIV prevalence in older adolescents and recent surveys include data on younger adolescents. Only a few countries have nationwide electronic case-based HIV surveillance, with the ability to provide population-level data on key HIV outcomes in the diagnosed population living with HIV. However, in the 15 highest adolescent HIV burden countries, there are no systems tracking adolescent transition to adulthood or healthcare transition. The strength of the 2016 WHO adolescent-specific recommendations on antiretroviral therapy and provision of HIV services to adolescents was hampered by the lack of evidence specific to this age group.
Progress is being made in national surveillance and global monitoring systems to specifically identify trends in adolescents living with HIV. However, HIV programmes responsive to the evolving HIV prevention and treatment needs of adolescents can be facilitated further by: data disaggregation to younger and older adolescents and mode of HIV infection where feasible; implementation of tools to achieve expanded national case-based surveillance; streamlining consent/assent procedures in younger adolescents and consensus on indicators of adolescent healthcare transition and transition to adulthood.
随着垂直感染艾滋病毒儿童存活率的提高以及新的水平传播艾滋病毒感染的持续发生,感染艾滋病毒的青少年(10至19岁)人数正在增加。本综述旨在描述青少年艾滋病毒流行的流行病学情况,以及国家监测系统在衡量艾滋病毒感染青少年从青少年期过渡到成年期的结果方面的能力。
利用2016年联合国艾滋病规划署的估计数据,对关键流行指标方面较年轻青少年(10至14岁)和较年长青少年(15至19岁)之间的全球趋势差异进行了研究。对15个青少年艾滋病毒负担最重国家基于全国人口的调查数据进行了评估,并介绍了国家个案监测系统的实例。最后,我们考虑了2016年世界卫生组织《关于使用抗逆转录病毒药物治疗和预防艾滋病毒感染的综合指南》中针对青少年的建议可能产生的影响。
联合国艾滋病规划署的估计表明,感染艾滋病毒的青少年人数正在增加,较年长青少年中的新艾滋病毒感染病例正在减少,虽然较年轻青少年中与艾滋病相关的死亡人数开始下降,但较年长青少年中的此类死亡人数仍在增加。基于全国人口的调查提供了较年长青少年艾滋病毒流行率的宝贵估计数据,最近的调查还包括了较年轻青少年的数据。只有少数国家拥有全国性的基于电子病例的艾滋病毒监测系统,能够提供感染艾滋病毒确诊人群关键艾滋病毒结果的人群水平数据。然而,在15个青少年艾滋病毒负担最重的国家,没有跟踪青少年向成年期过渡或医疗保健过渡的系统。2016年世界卫生组织关于抗逆转录病毒疗法和为青少年提供艾滋病毒服务的针对青少年的建议,因缺乏该年龄组的具体证据而受到阻碍。
国家监测和全球监测系统在具体确定感染艾滋病毒青少年的趋势方面正在取得进展。然而,通过以下方式可进一步推动满足青少年不断变化的艾滋病毒预防和治疗需求的艾滋病毒项目:在可行的情况下按较年轻和较年长青少年以及艾滋病毒感染方式进行数据分类;实施工具以实现扩大的国家个案监测;简化较年轻青少年的同意/赞成程序,并就青少年医疗保健过渡和向成年期过渡的指标达成共识。