Zwahlen Diana, Tondorf Theresa, Rothschild Sacha, Koller Michael T, Rochlitz Christoph, Kiss Alexander
Department of Psychosomatic Medicine, University Hospital Basel, Hebelstrasse 2, 4031, Basel, Switzerland.
Medical Oncology Department, University Hospital Basel, Petersgraben 4, 4031, Basel, Switzerland.
BMC Cancer. 2017 May 30;17(1):385. doi: 10.1186/s12885-017-3362-x.
International standards prioritize introducing routine emotional distress screening in cancer care to accurately identify patients who most need psycho-oncological treatment, and ensure that patients can access appropriate supportive care. However, only a moderate proportion of distressed patients accepts referrals to or uses psycho-oncological support services. Predictors and barriers to psycho-oncological support service utilization are under-studied. We know little about how patients and oncologists perceive the discussions when oncologists assess psychosocial distress with a screening instrument. We aim to 1) assess the barriers and predictors of uptake of in-house psycho-oncological support along the distress screening pathway in cancer patients treated at a University Oncology Outpatient Clinic and, 2) determine how patients and clinicians perceive communication about psychosocial distress after screening with the Distress Thermometer.
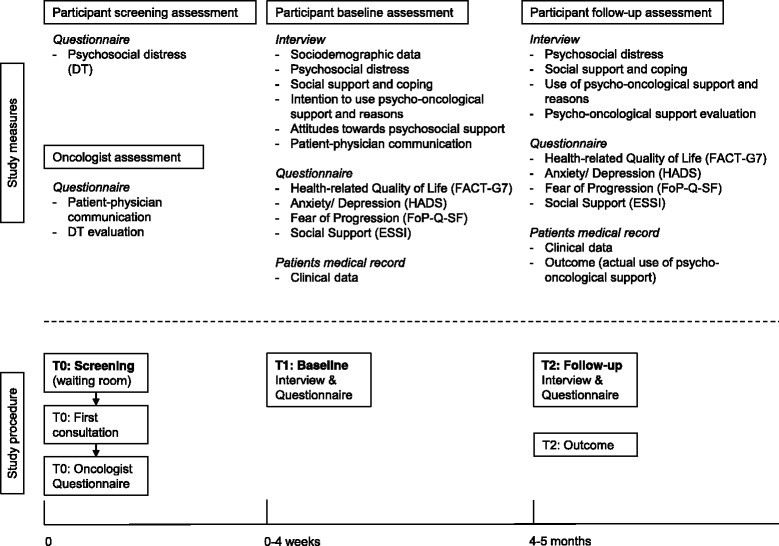
This is a quantitative prospective observational study with qualitative aspects. We will examine medical and demographic variables, cancer patient self-reports of various psychological measures, and aspects of the patient-clinician communication as variables that potentially predict uptake of psycho-oncological support service. We will also assess the patients' reasons for accepting or refusing psycho-oncological support services. We assess at three points in time, based on paper-and-pencil questionnaires and two patient interviews during the study period. We will monitor outcomes (psycho-oncology service uptake) four months after study entry.
The study will improve our understanding of characteristics of patients who accept or refuse psycho-oncological support, and help us understand how patients' and oncologists perceive communication about psychosocial distress, and referral to a psycho-oncologist. We believe this is the first study to focus on factors that affect uptake or rejection of psycho-oncological support services along the screening and referral pathway. The study 1) combines standard assessment with qualitative data collection, 2) embraces patient and oncologist perspectives, and, 3) focuses on patient-clinician communication about psychosocial issues raised by a standard screening instrument. Our results may improve routine practices and eliminate barriers to adequate health care, and make it easier to recognize patients with high distress levels who underuse the service.
国际标准将在癌症护理中引入常规情绪困扰筛查作为优先事项,以准确识别最需要心理肿瘤治疗的患者,并确保患者能够获得适当的支持性护理。然而,只有一部分感到困扰的患者接受转介或使用心理肿瘤支持服务。心理肿瘤支持服务利用的预测因素和障碍研究不足。我们对患者和肿瘤学家在肿瘤学家使用筛查工具评估心理社会困扰时对讨论的看法知之甚少。我们旨在:1)评估在大学肿瘤门诊接受治疗的癌症患者在困扰筛查过程中接受内部心理肿瘤支持的障碍和预测因素;2)确定患者和临床医生在用苦恼温度计筛查后对心理社会困扰沟通的看法。
这是一项兼具定量和定性方面的前瞻性观察性研究。我们将检查医学和人口统计学变量、癌症患者对各种心理测量的自我报告以及患者与临床医生沟通的方面,将其作为可能预测心理肿瘤支持服务利用情况的变量。我们还将评估患者接受或拒绝心理肿瘤支持服务的原因。在研究期间,我们基于纸笔问卷和两次患者访谈在三个时间点进行评估。我们将在研究开始四个月后监测结果(心理肿瘤服务利用情况)。
该研究将增进我们对接受或拒绝心理肿瘤支持的患者特征的理解,并帮助我们了解患者和肿瘤学家对心理社会困扰沟通以及转介给心理肿瘤学家的看法。我们认为这是第一项关注筛查和转介过程中影响心理肿瘤支持服务接受或拒绝因素的研究。该研究:1)将标准评估与定性数据收集相结合;2)涵盖患者和肿瘤学家的观点;3)关注患者与临床医生就标准筛查工具提出的心理社会问题进行的沟通。我们的结果可能会改善常规做法,消除获得充分医疗保健的障碍,并使更容易识别那些未充分利用该服务的高度困扰患者。