Obermeier Juliane, Trefz Phillip, Happ Josephine, Schubert Jochen K, Staude Hagen, Fischer Dagmar-Christiane, Miekisch Wolfram
Department of Anesthesiology and Intensive Care Medicine, Rostock Medical Breath Research Analytics and Technologies (ROMBAT), University Medicine Rostock, Rostock, Germany.
Department of Pediatrics, University Medicine Rostock, Rostock, Germany.
PLoS One. 2017 Jun 1;12(6):e0178745. doi: 10.1371/journal.pone.0178745. eCollection 2017.
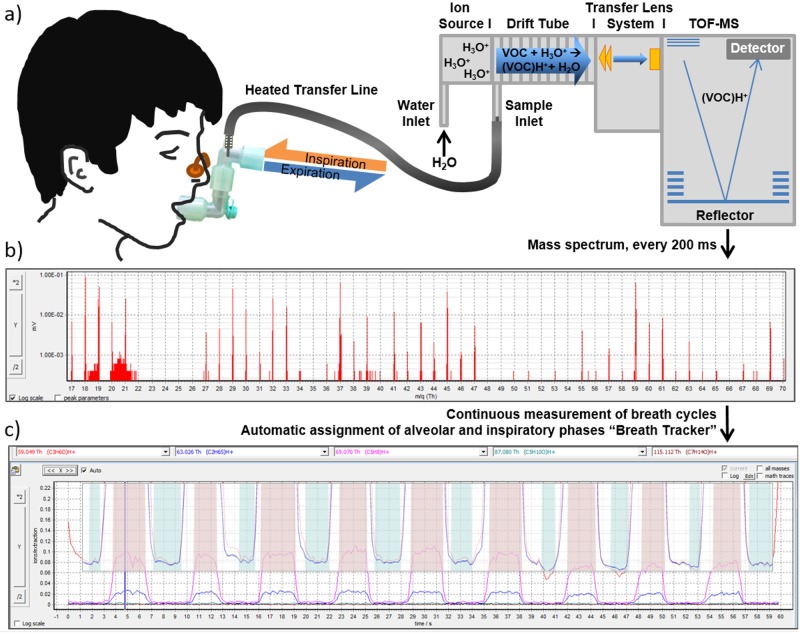
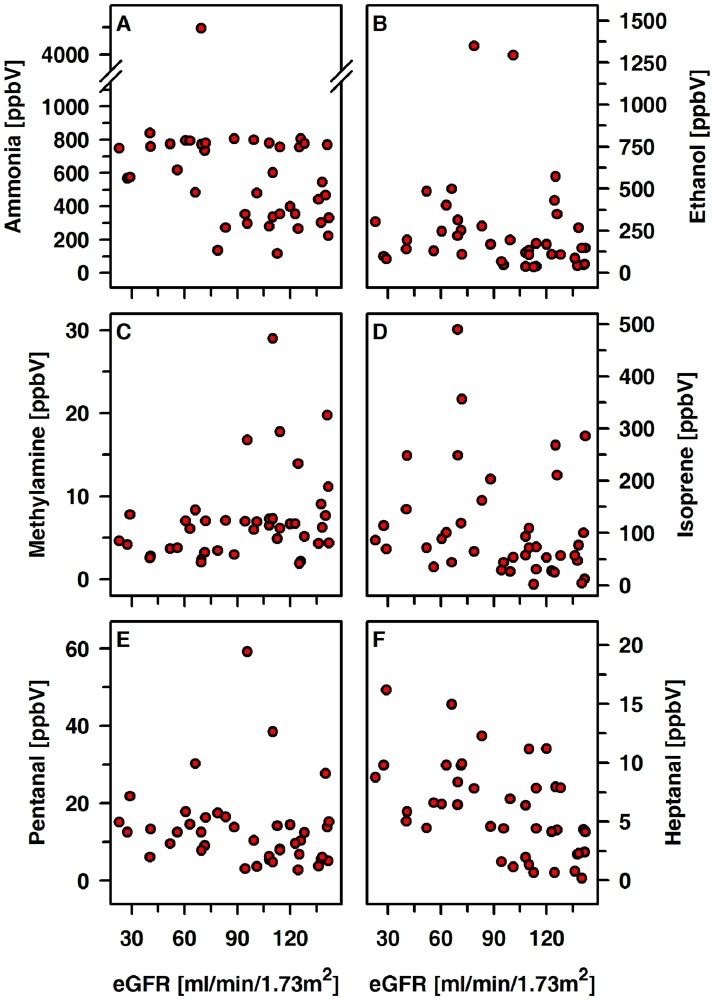
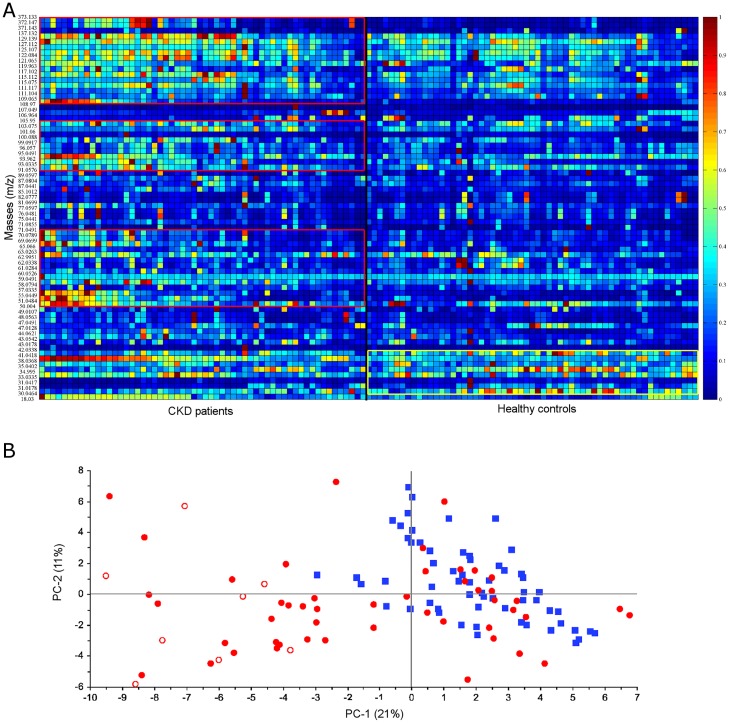
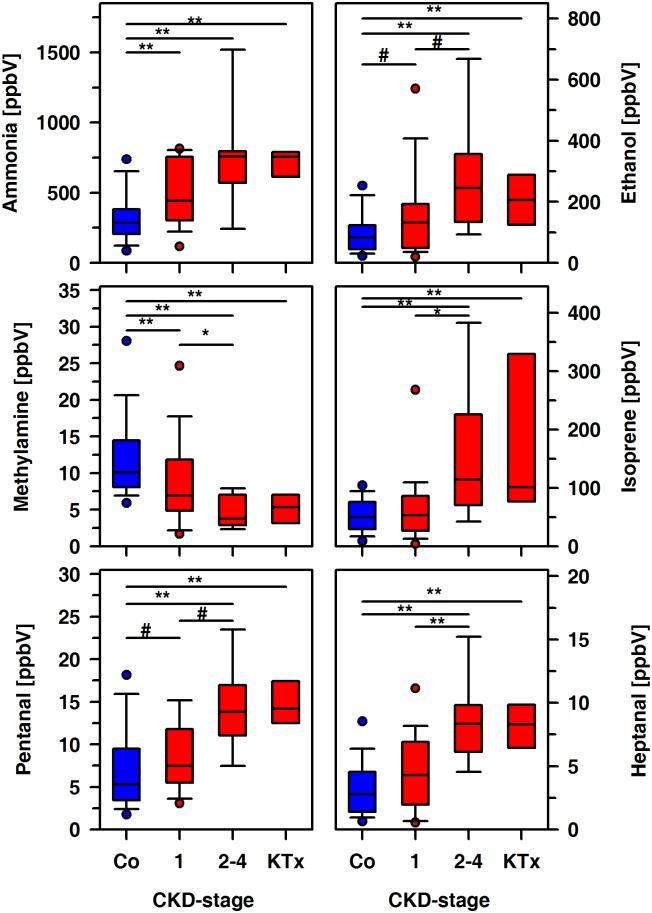
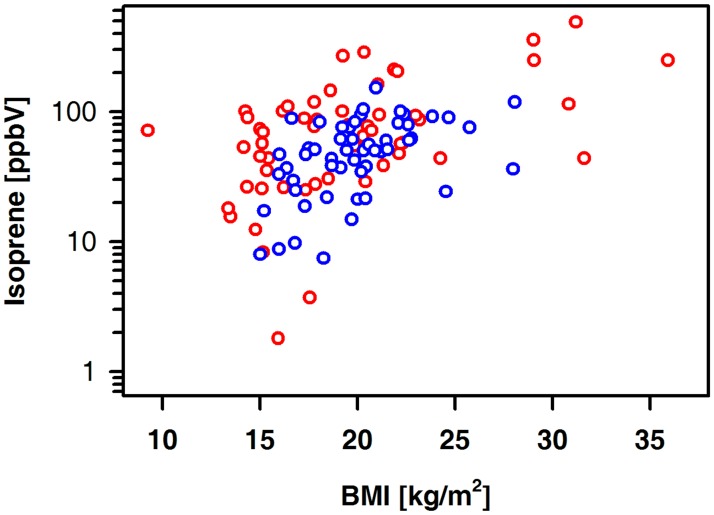
Monitoring metabolic adaptation to chronic kidney disease (CKD) early in the time course of the disease is challenging. As a non-invasive technique, analysis of exhaled breath profiles is especially attractive in children. Up to now, no reports on breath profiles in this patient cohort are available. 116 pediatric subjects suffering from mild-to-moderate CKD (n = 48) or having a functional renal transplant KTx (n = 8) and healthy controls (n = 60) matched for age and sex were investigated. Non-invasive quantitative analysis of exhaled breath profiles by means of a highly sensitive online mass spectrometric technique (PTR-ToF) was used. CKD stage, the underlying renal disease (HUS; glomerular diseases; abnormalities of kidney and urinary tract or polycystic kidney disease) and the presence of a functional renal transplant were considered as classifiers. Exhaled volatile organic compound (VOC) patterns differed between CKD/ KTx patients and healthy children. Amounts of ammonia, ethanol, isoprene, pentanal and heptanal were higher in patients compared to healthy controls (556, 146, 70.5, 9.3, and 5.4 ppbV vs. 284, 82.4, 49.6, 5.30, and 2.78 ppbV). Methylamine concentrations were lower in the patient group (6.5 vs 10.1 ppbV). These concentration differences were most pronounced in HUS and kidney transplanted patients. When patients were grouped with respect to degree of renal failure these differences could still be detected. Ammonia accumulated already in CKD stage 1, whereas alterations of isoprene (linked to cholesterol metabolism), pentanal and heptanal (linked to oxidative stress) concentrations were detectable in the breath of patients with CKD stage 2 to 4. Only weak associations between serum creatinine and exhaled VOCs were noted. Non-invasive breath testing may help to understand basic mechanisms and metabolic adaptation accompanying progression of CKD. Our results support the current notion that metabolic adaptation occurs early during the time course of CKD.
在慢性肾脏病(CKD)病程早期监测其代谢适应性具有挑战性。作为一种非侵入性技术,分析呼出气成分对儿童尤其具有吸引力。到目前为止,尚无关于该患者队列呼出气成分的报告。本研究调查了116名儿科受试者,其中包括患有轻至中度CKD的儿童(n = 48)、接受功能性肾移植(KTx)的儿童(n = 8)以及年龄和性别匹配的健康对照儿童(n = 60)。采用高灵敏度在线质谱技术(PTR-ToF)对呼出气成分进行非侵入性定量分析。将CKD分期、潜在的肾脏疾病(溶血尿毒综合征;肾小球疾病;肾脏和尿路异常或多囊肾病)以及功能性肾移植的存在作为分类因素。CKD/KTx患者与健康儿童的呼出气挥发性有机化合物(VOC)模式存在差异。与健康对照相比,患者呼出的氨、乙醇、异戊二烯、戊醛和庚醛含量更高(分别为556、146、70.5、9.3和5.4 ppbV,而健康对照分别为284、82.4、49.6、5.30和2.78 ppbV)。患者组中甲胺浓度较低(6.5 vs 10.1 ppbV)。这些浓度差异在溶血尿毒综合征患者和肾移植患者中最为明显。当根据肾衰竭程度对患者进行分组时,这些差异仍然可以检测到。氨在CKD 1期就已积累,而异戊二烯(与胆固醇代谢有关)、戊醛和庚醛(与氧化应激有关)浓度的变化在CKD 2至4期患者的呼出气中可检测到。血清肌酐与呼出VOCs之间仅存在微弱关联。非侵入性呼气测试可能有助于了解CKD进展过程中的基本机制和代谢适应性。我们的结果支持目前的观点,即代谢适应性在CKD病程早期就已发生。