Raykar Nakul P, Yorlets Rachel R, Liu Charles, Goldman Roberta, Greenberg Sarah L M, Kotagal Meera, Farmer Paul E, Meara John G, Roy Nobhojit, Gillies Rowan D
Program in Global Surgery and Social Change, Harvard Medical School, Boston, Massachusetts, USA.
Beth Israel Deaconess Medical Center, Boston, Massachusetts, USA.
BMJ Glob Health. 2016 Dec 16;1(4):e000075. doi: 10.1136/bmjgh-2016-000075. eCollection 2016.
5 billion people around the world do not have access to safe, affordable, timely surgical care. This series of qualitative interviews was launched by The Commission on Global Surgery (LCoGS) with the aim of understanding the contextual challenges-the specific circumstances-faced by surgical care providers in low-resource settings who care for impoverished patients, and how those providers overcome these challenges.
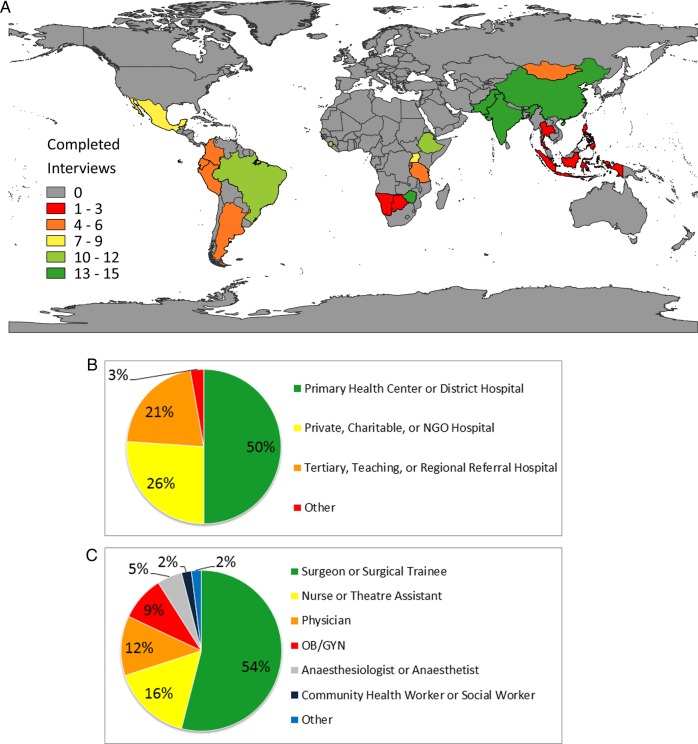
From January 2014 to February 2015, 20 LCoGS collaborators conducted semistructured interviews with 148 surgical providers in low-resource settings in 21 countries. Stratified purposive sampling was used to include both rural and urban providers, and reputational case selection identified individuals. Interviewers were trained with an implementation manual. Following immersion into de-identified texts from completed interviews, topical coding and further analysis of coded texts was completed by an independent analyst with periodic validation from a second analyst.
Providers described substantial financial, geographic and cultural barriers to patient access. Rural surgical teams reported a lack of a trained workforce and insufficient infrastructure, equipment, supplies and banked blood. Urban providers face overcrowding, exacerbated by minimal clinical and administrative support, and limited interhospital care coordination. Many providers across contexts identified national health policies that do not reflect the realities of resource-poor settings. Some findings were region-specific, such as weak patient-provider relationships and unreliable supply chains. In all settings, surgical teams have created workarounds to deliver care despite the challenges.
While some differences exist between countries, the barriers to safe surgery and anaesthesia are overall consistent and resource-dependent. Efforts to advance and expand global surgery must address these commonalities, while local policymakers can tailor responses to key contextual differences.
全球有50亿人无法获得安全、可负担、及时的外科治疗。全球外科委员会(LCoGS)开展了这一系列定性访谈,旨在了解在资源匮乏地区为贫困患者提供治疗的外科护理人员所面临的背景挑战——具体情况,以及这些人员如何克服这些挑战。
2014年1月至2015年2月,20名LCoGS合作者对21个国家资源匮乏地区的148名外科护理人员进行了半结构化访谈。采用分层目的抽样法纳入农村和城市的护理人员,并通过声誉案例选择确定访谈对象。访谈人员接受了实施手册培训。在深入研究已完成访谈的匿名文本后,由一名独立分析师完成主题编码和对编码文本的进一步分析,并由第二名分析师定期进行验证。
护理人员描述了患者就医面临的重大财务、地理和文化障碍。农村外科团队报告称缺乏训练有素的劳动力,基础设施、设备、物资和储备血不足。城市护理人员面临过度拥挤的问题,临床和行政支持极少以及医院间护理协调有限使这一问题更加严重。许多不同背景的护理人员都指出国家卫生政策未能反映资源匮乏地区的实际情况。一些研究结果具有地区特殊性,比如医患关系薄弱和供应链不可靠。在所有情况下,外科团队都在尽管面临挑战的情况下想出了变通办法来提供护理。
虽然各国之间存在一些差异,但安全手术和麻醉的障碍总体上是一致的,且依赖于资源。推进和扩大全球外科手术的努力必须解决这些共性问题,而地方政策制定者可以针对关键的背景差异调整应对措施。