Ghodsi Saeed, Meysamie Alipasha, Abbasi Mehrshad, Ghalehtaki Reza, Esteghamati Alireza, Malekzadeh Masoud M, Asgari Fereshteh, Gouya Mohammad M
Department of Community and Preventive Medicine, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
Endocrinology and Metabolism Research Center (EMRC), Vali-Asr Hospital, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
J Diabetes Metab Disord. 2017 Jun 7;16:25. doi: 10.1186/s40200-017-0306-6. eCollection 2017.
Non-HDL-C as a valuable predictor of premature atherosclerosis, coronary events like first Myocardial infarction and cardiovascular mortality has a high accuracy of measurement both in fasting and non-fasting individuals. Metabolic syndrome (MetS) can promote the development of diabetes mellitus, endothelial dysfunction and atherosclerosis. A common pathway for cross linking of metabolic abnormalities and non-HDL-C has been suggested. In this study we aimed to describe the potential association between non-HDL cholesterol fractions and metabolic syndrome.
Data of third national surveillance of the risk factors of non-communicable diseases (SuRFNCD-2007) were analyzed. We defined metabolic syndrome (MetS) according to the Adult Treatment Panel III (ATPIII) and International Diabetes Federation (IDF) criteria for 2125 subjects aging 25-64 years. The receiver operating characteristic (ROC) curves were used to determine the optimal cut-points for the diagnosis of MetS. The curves were depicted for non-high-density lipoprotein cholesterol (non-HDL-C) and difference of total non-HDL-C and LDL-C (Differential cholesterol or Diff-C) as predictors of MetS. Logistic regression was also performed in a complex sample analysis scheme.
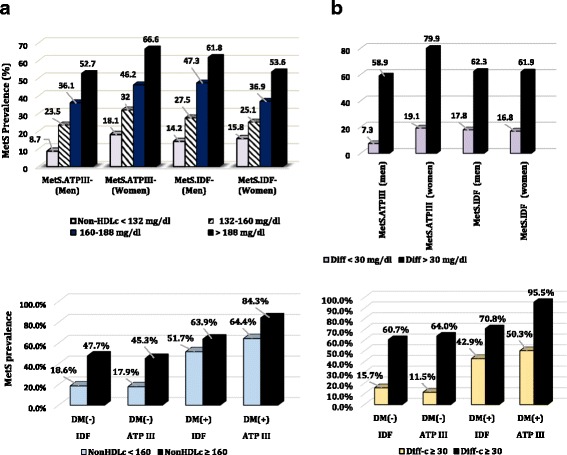
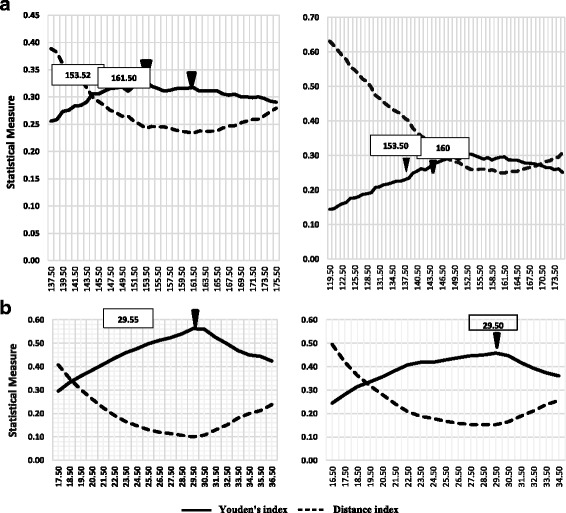
The area under the curve (AUC) with 95% Confidence intervals of total non-HDL-C was computed. Values were 0.693 (0.670-0.715) for IDF-defined MetS and 0.719 (0.697-0.740) for ATPIII criteria. The optimal non-HDL-C cut-point we recommend for both criteria is 153.50 mg/dl (sensitivity: 75.7%, specificity: 57.2%, with ATPIII; sensitivity: 73.2%, specificity: 57.1%, with IDF). Using IDF criteria, the accuracy of predictors were greater in non-diabetic subjects. AUC of Diff-C in DM (-) vs. DM (+) were 0.786 (0.765-0.807) vs. 0.627(0.549-0.705). Adults with high non-HDL-C were 4.42 times more likely to have ATPIII-defined MetS (≥190 vs. < 190 mg/dL). Elevated Diff-C corresponded to increased risk of the MetS (ORs: 10.71 and 26.29 for IDF and ATP III criteria, respectively. All -values <0.001).
A significant robust association exists between non-HDL-C and MetS whether applying conventional or new thresholds.
非高密度脂蛋白胆固醇(Non-HDL-C)作为过早动脉粥样硬化、首次心肌梗死等冠状动脉事件及心血管死亡率的重要预测指标,在空腹和非空腹个体中均具有较高的测量准确性。代谢综合征(MetS)可促进糖尿病、内皮功能障碍和动脉粥样硬化的发展。已有研究提出了代谢异常与非高密度脂蛋白胆固醇之间的共同联系途径。在本研究中,我们旨在描述非高密度脂蛋白胆固醇各组分与代谢综合征之间的潜在关联。
分析第三次全国非传染性疾病危险因素监测(SuRFNCD - 2007)的数据。我们根据成人治疗小组第三次报告(ATPIII)和国际糖尿病联盟(IDF)标准,对2125名年龄在25 - 64岁的受试者定义代谢综合征(MetS)。采用受试者工作特征(ROC)曲线确定代谢综合征诊断的最佳切点。绘制以非高密度脂蛋白胆固醇(non-HDL-C)以及总非高密度脂蛋白胆固醇与低密度脂蛋白胆固醇差值(差异胆固醇或Diff-C)作为代谢综合征预测指标的曲线。还采用复杂样本分析方案进行逻辑回归分析。
计算了总非高密度脂蛋白胆固醇曲线下面积(AUC)及其95%置信区间。IDF定义的代谢综合征的AUC值为0.693(0.670 - 0.715),ATPIII标准的AUC值为0.719(0.697 - 0.740)。我们推荐的两种标准下的最佳非高密度脂蛋白胆固醇切点均为153.50mg/dl(ATPIII标准下的敏感性:75.7%,特异性:57.2%;IDF标准下的敏感性:73.2%,特异性:57.1%)。采用IDF标准时,非糖尿病受试者中预测指标的准确性更高。糖尿病患者(DM(-))与糖尿病患者(DM(+))中Diff-C的AUC分别为0.786(0.765 - 0.807)和0.627(0.549 - 0.705)。非高密度脂蛋白胆固醇水平高的成年人患ATPIII定义的代谢综合征(≥190 vs. < 190mg/dL)的可能性高4.42倍。Diff-C升高与代谢综合征风险增加相关(IDF和ATP III标准下的比值比分别为10.71和26.29。所有P值<0.001)。
无论采用传统阈值还是新阈值,非高密度脂蛋白胆固醇与代谢综合征之间均存在显著且稳健的关联。